

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Gastric polyps encompass a wide variety of lesions that most commonly arise from the gastric epithelium. However, coincidental gastric carcinomas have rarely been reported, being found in only 2~3% of patients with hyperplastic polyps. A 68-year-old male was admitted to our hospital for bleeding control of a gastric polyp. The gastroscopy shows numerous polyps in the entire gastric mucosa and a huge ulcer with bleeding. The bleeding of the gastric ulcer could not be controlled by gastroscopic procedures. So, we performed total gastrectomy for bleeding control. The pathologic findings shows poorly differentiated adenocarcinoma with hyperplastic polyps. We performed treatment with Cisplatin and 5-FU for two cycles. Two months postoperative, he was admitted due to dyspnea associated with ascites. We performed a ckeckup by computer tomography. It revealed cancer recurrence with lymphatic and liver metastasis, and diffuse massive ascites with mesenteric cake, and it suggested cancer peritonei.
Figures and Tables
Fig. 1
Gastroscopy shows bloody oozing on the ulcerative lesion (A) and multiple polyps on the gastric wall (B).

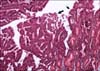
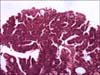
Fig. 2
Gross finding; This shows multiple polyps on whole gastric epithelium and huge ulcerative lesion.


References
1. Niv Y, Delpre G, Sperber AD, Sandbank J, Zirkin H. Hyperplastic gastric polyposis, hypergastrinaemia and colorectal neoplasia: a description of four cases. Eur J Gastroenterol Hepatol. 2003. 15:1361–1366.
2. Kozuka S, Masamoto K, Suzuki S, Kubota K, Yokoyama Y. Histogenetic types and size of polypoid lesions in the stomach, with special reference to cancerous change. Gann. 1977. 68:267–274.
3. Oberhuber G, Stolte M. Gastric polyps: an update of their pathology and biological significance. Virchows Arch. 2000. 437:581–590.
4. Ming SC, Goldman H. Pathology of the Gastrointestinal Tract. 1992. 1st ed. Philadelphia: Saunders.
5. Hattori T. Morphological range of hyperplastic polyps and carcinomas arising in hyperplastic polyps of the stomach. J Clin Pathol. 1985. 38:622–630.
6. Orlowska J, Jarosz D, Pachlewski J, Butruk E. Malignant transformation of benign epithelial gastric polyps. Am J Gastroenterol. 1995. 90:2152–2159.
7. Zea-Iriarte WL, Sekine I, Itsuno M, Makiyama K, Naito S, Nakayama T, et al. Carcinoma in gastric hyperplastic polyps. A phenotypic study. Dig Dis Sci. 1996. 41:377–386.
8. Nakamura T, Nakano G. Histopathological classification and malignant change in gastric polyps. J Clin Pathol. 1985. 38:754–764.
9. Sung HY, Cheung DY, Cho SH, Kim JI, Park SH, Han JY, et al. Polyps in the gastrointestinal tract: discrepancy between endoscopic forceps biopsies and resected specimens. Eur J Gastroenterol Hepatol. 2009. 21:190–195.
10. Murakami R, Tsukuma H, Kanamori S, Imanishi K, Otani T, Nakanishi K, et al. Natural history of colorectal polyps and the effect of polypectomy on occurrence of subsequent cancer. Int J Cancer. 1990. 46:159–164.
 XML Download
XML Download