

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Focal aneurysmal change after spontaneous superior mesenteric artery (SMA) dissection has been reported rarely. A stent graft implantation can exclude false lumen and possibly make major abdominal operation avoidable. A 52-year-old male patient was admitted due to abdominal pain for 10 days. A CT scan showed severe narrowing of the true lumen of SMA, approximately a 7 cm segment from the origin, due to compression by the thrombosed false lumen. Five days after admission, abdominal pain aggravated progressively. The follow-up CT revealed focal aneurysmal dilatation of the dissected SMA segment. I report here an endovascular treatment with stent graft implantation for a focal aneurysmal change after SMA dissection.
Figures and Tables
Fig. 1
Diffuse narrowing of the true lumen by thrombosed false lumen (white arrow) is noted. Intimal flap and stenosis on right common iliac artery is visible (dot arrow). Distension of stomach (arrow head) is noted.

Fig. 2
Computed tomography angiography demonstrates a focal SMA aneurysmal change (white arrow), diffuse narrowing of the true lumen (dot arrow) by thrombosed false lumen (arrow head).

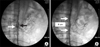
Fig. 3
(A) Selective angiogram of the SMA shows dissection of the main trunk of the SMA with true (black arrows) and false (white arrows) lumens. (B) Post-stent graft (white arrow) implantation angiogram of SMA with complete exclusion of the false lumen.


References
1. Bauersfeld SR. Dissecting aneurysm of the aorta: a presentation of fifteen cases and a review of the recent literature. Ann Intern Med. 1947. 26:873–889.
2. Wu XM, Wang TD, Chen MF. Percutaneous endovascular treatment for isolated spontaneous superior mesenteric artery dissection: report of two cases and literature review. Catheter Cardiovasc Interv. 2009. 73:145–151.
3. Kim JH, Roh BS, Lee YH, Choi SS, So BJ. Isolated spontaneous dissection of the superior mesenteric artery: percutaneous stent placement in two patients. Korean J Radiol. 2004. 5:134–138.
4. Chang HJ, Yang KH, Lee WY, Bae BN, Kim KH, Han S, et al. Traumatic isolated SMA dissecting aneurysm associated with burst fractures of lumbar spines. J Korean Soc Vasc Surg. 2007. 23:62–66.
5. Goueffic Y, Costargent A, Dupas B, Heymann MF, Chaillou P, Patra P. Superior mesenteric artery dissection: case report. J Vasc Surg. 2002. 35:1003–1005.
6. Solis MM, Ranval TJ, McFarland DR, Eidt JF. Surgical treatment of superior mesenteric artery dissecting aneurysm and simultaneous celiac artery compression. Ann Vasc Surg. 1993. 7:457–462.
7. Yun WS, Kim YW, Park KB, Cho SK, Do YS, Lee KB, et al. Clinical and angiographic follow-up of spontaneous isolated superior mesenteric artery dissection. Eur J Vasc Endovasc Surg. 2009. 37:572–577.
8. Yoon YW, Choi D, Cho SY, Lee DY. Successful treatment of isolated spontaneous superior mesenteric artery dissection with stent placement. Cardiovasc Intervent Radiol. 2003. 26:475–478.
9. Sparks SR, Vasquez JC, Bergan JJ, Owens EL. Failure of nonoperative management of isolated superior mesenteric artery dissection. Ann Vasc Surg. 2000. 14:105–109.
 XML Download
XML Download