

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Inflammatory myofibroblastic tumor (IMT) is an uncommon tumor which is composed of spindle cells admixed with mature plasma cells and inflammatory cells. IMT is most common in the lungs and in various organs. However, it is very rare in the breast. According to the organ, there are many clinical and histological characteristics. Breast IMT usually shows developed, movable nontender mass. Radiological findings of IMT are similar to primary breast malignancy. For accurate diagnosis, histologic correlation is needed. IMT is a benign lesion and excision is the treatment of choice, but wide local excision and negative resection margin is needed due to its tendency for recurrence. Understanding of the entity and its mimicry can be helpful in avoiding any unnecessary surgical procedures, such as mastectomy with or without lymph node dissection. Herein, the case of a 29-year-old woman found to have IMT of the breast. The patient underwent a wide local excision. The gross, microscopic and immunohistochemical findings were consistent with the diagnosis of IMT of the breast.
Figures and Tables
Fig. 1
Right breast ultrasonogram: Ultrasonogram demonstrates an ill defined, homogenous, hypoechoic 2 cm sized septated mass in right breast at 12 o'clock.
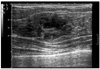
Fig. 2
Microscopic findings of inflammatory myofibroblastic tumor: Ill-defined tumor shows infiltrative proliferation of spindle cells (H&E stain, ×100).
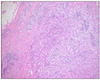
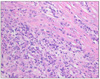
Fig. 3
Microscopic findings of inflammatory myofibroblastic tumor: The tumor is composed of spindle cells and inflammatory cells including foamy histiocytes, lymphocytes, and plasma cells (H&E stain, ×400).

References
1. Coffin CM, Humphrey PA, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor: a clinical and pathological survey. Semin Diagn Pathol. 1998. 15:85–101.
2. Pettinato G, Manivel JC, Insabato L, De Chiara A, Petrella G. Plasma cell granuloma (inflammatory pseudotumor) of the breast. Am J Clin Pathol. 1988. 90:627–632.
3. Pettinato G, Manivel JC, De Rosa N, Dehner LP. Inflammatory myofibroblastic tumor (plasma cell granuloma). Clinicopathologic study of 20 cases with immunohistochemical and ultrastructural observations. Am J Clin Pathol. 1990. 94:538–546.
4. Coffin CM, Watterson J, Priest JR, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor). A clinicopathologic and immunohistochemical study of 84 cases. Am J Surg Pathol. 1995. 19:859–872.
5. Park IK, Yoon DS, Kim YM, Park HD, Min SK. Inflammatory myofibroblastic tumor of the breast. J Breast Cancer. 2006. 9:258–261.
6. Zardawi IM, Clark D, Williamsz G. Inflammatory myofibroblastic tumor of the breast. A case report. Acta Cytol. 2003. 47:1077–1081.
7. Sastre-Garau X, Couturier J, Derre J, Aurias A, Klijanienko J, Lagace R. Inflammatory myofibroblastic tumour (inflammatory pseudotumour) of the breast. Clinicopathological and genetic analysis of a case with evidence for clonality. J Pathol. 2002. 196:97–102.
8. Ilvan S, Celik V, Paksoy M, Cetinaslan I, Calay Z. Inflammatory myofibroblastic tumor (inflammatory pseudotumor) of the breast. APMIS. 2005. 113:66–69.
9. Khanafshar E, Phillipson J, Schammel DP, Minobe L, Cymerman J, Weidner N. Inflammatory myofibroblastic tumor of the breast. Ann Diagn Pathol. 2005. 9:123–129.
10. Zen Y, Kasahara Y, Horita K, Miyayama S, Miura S, Kitagawa S, et al. Inflammatory pseudotumor of the breast in a patient with a high serum IgG4 level: histologic similarity to sclerosing pancreatitis. Am J Surg Pathol. 2005. 29:275–278.
 XML Download
XML Download