

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We aimed to evaluate the early (<30 days) results and to analyze risk factors for the development of stroke and new brain infarction (NBI) after carotid endarterectomy (CEA).
Methods
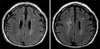
From September 2003 to August 2008, 233 CEAs were performed on 222 patients with critical internal carotid artery (ICA) stenosis in a single center. Patient characteristics, history of neurological symptoms, procedural details, and postoperative complications were examined based on the medical records. The incidence and risk factors for early postoperative stroke were evaluated. After excluding CEAs without performing diffusion-weighted brain MRI, 128 CEAs were investigated for frequency and the risk factors of NBI were analyzed. Chi-square test, Fisher's exact test, Student T-test, and logistic regression model were used for statistical analysis.
Results
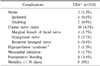
Of a total of 233 CEAs, any and ipsilateral stroke rates were 1.3% and 0.4%, respectively. There was no early postoperative mortality. Early postoperative complications included 4.3% in transient cranial nerve injury, 1.7% in myocardial infarction, and 3.4% in hematoma. In univariate analysis, the significant risk factor for stroke was plaque ulceration (P=0.04). The frequency of NBI and ipsilateral NBI were 8.4% and 3.1%, respectively. The ulceration on ipsilateral ICA revealed statistically significant risk factors for the development of NBI (RR, 5.29; 95% CI, 1.024~27.325; P=0.04).
Conclusion
Our study showed a lower incidence of stroke and NBI after carotid endarterectomy and that it is safe procedure for the treatment of patients with severe (>70%) carotid stenosis. We also found that plaque with ulceration was a significant risk factor for the development of postoperative NBI.
Figures and Tables




References
1. Murray CJ, Lopez AD. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet. 1997. 349:1269–1276.
2. Thrift AG, Dewey HM, Macdonell RA, McNeil JJ, Donnan GA. Incidence of the major stroke subtypes: initial findings from the North East Melbourne stroke incidence study (NEMESIS). Stroke. 2001. 32:1732–1738.
3. Chaturvedi S, Bruno A, Feasby T, Holloway R, Benavente O, Cohen SN, et al. Carotid endarterectomy--an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2005. 65:794–801.
4. Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954. 267:994–996.
5. Biller J, Feinberg WM, Castaldo JE, Whittemore AD, Harbaugh RE, Dempsey RJ, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation. 1998. 97:501–509.
6. Matsen SL, Chang DC, Perler BA, Roseborough GS, Williams GM. Trends in the in-hospital stroke rate following carotid endarterectomy in California and Maryland. J Vasc Surg. 2006. 44:488–495.
7. McPhee JT, Hill JS, Ciocca RG, Messina LM, Eslami MH. Carotid endarterectomy was performed with lower stroke and death rates than carotid artery stenting in the United States in 2003 and 2004. J Vasc Surg. 2007. 46:1112–1118.
8. Kasner SE. Clinical interpretation and use of stroke scales. Lancet Neurol. 2006. 5:603–612.
9. Thygesen K, Alpert JS, White HD. Joint ESC/ACCF/AHA/ WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. Circulation. 2007. 116:2634–2653.
10. North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991. 325:445–453.
11. European Carotid Surgery Trialists' Collaborative Group. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998. 351:1379–1387.
12. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. Endarterectomy for asymptomatic carotid artery stenosis. JAMA. 1995. 273:1421–1428.
13. Halliday A, Mansfield A, Marro J, Peto C, Peto R, Potter J, et al. MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet. 2004. 363:1491–1502.
14. Mas JL, Chatellier G, Beyssen B, Branchereau A, Moulin T, Becquemin JP, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006. 355:1660–1671.
15. Halm EA, Tuhrim S, Wang JJ, Rockman C, Riles TS, Chassin MR. Risk factors for perioperative death and stroke after carotid endarterectomy: results of the New York carotid artery surgery study. Stroke. 2009. 40:221–229.
16. Rockman CB, Su W, Lamparello PJ, Adelman MA, Jacobowitz GR, Gagne PJ, et al. A reassessment of carotid endarterectomy in the face of contralateral carotid occlusion: surgical results in symptomatic and asymptomatic patients. J Vasc Surg. 2002. 36:668–673.
17. Mackey WC. Carotid and coronary disease: staged or simultaneous management? Semin Vasc Surg. 1998. 11:36–40.
18. Kolh PH, Comte L, Tchana-Sato V, Honore C, Kerzmann A, Mauer M, et al. Concurrent coronary and carotid artery surgery: factors influencing perioperative outcome and long-term results. Eur Heart J. 2006. 27:49–56.
19. Rockman CB, Halm EA, Wang JJ, Chassin MR, Tuhrim S, Formisano P, et al. Primary closure of the carotid artery is associated with poorer outcomes during carotid endarterectomy. J Vasc Surg. 2005. 42:870–877.
20. Bond R, Rerkasem K, AbuRahma AF, Naylor AR, Rothwell PM. Patch angioplasty versus primary closure for carotid endarterectomy. Cochrane Database Syst Rev. 2004. CD000160.
21. Lacroix V, Hammer F, Astarci P, Duprez T, Grandin C, Cosnard G, et al. Ischemic cerebral lesions after carotid surgery and carotid stenting. Eur J Vasc Endovasc Surg. 2007. 33:430–435.
22. Zukowski AJ, Nicolaides AN, Lewis RT, Mansfield AO, Williams MA, Helmis E, et al. The correlation between carotid plaque ulceration and cerebral infarction seen on CT scan. J Vasc Surg. 1984. 1:782–786.
23. Schnaudigel S, Groschel K, Pilgram SM, Kastrup A. New brain lesions after carotid stenting versus carotid endarterectomy: a systematic review of the literature. Stroke. 2008. 39:1911–1919.
 XML Download
XML Download