

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Idiopathic granulomatous mastitis is a rare benign inflammatory breast disease of an unknown etiology and the optimal treatment remains controversial. The aim of this study is to evaluate the efficacy of surgically complete excision in patients with idiopathic granulomatous mastitis.
Methods
Between March 2005 and November 2008, we treated 14 cases that were diagnosed with idiopathic granulomatous mastitis. Prospectively, we treated the cases with complete surgical excision with or without steroid therapy in all patients.
Results
The mean age of the patients was 36 years (range 30 to 53 years). All cases performed were complete excision with or without steroid therapy. The median follow up period was 26 months (range 5 to 50 months) and all cases had no recurrence. 13 patients out of the 14 were satisfied with the cosmesis of the treated breast.
Figures and Tables

 | Fig. 2Presentation of patient described in case 2, who had steroid therapy already. (A) View of the right breast in an idiopathic granulomatous mastitis with fistula formation. (B) The incision of periareolar and the skin lesion of fistula. (C) View of the specimen that has well demarcated margin.
|
 | Fig. 3(A) Ultrasonography before steroid therapy. (B) Ultrasonography after steroid therapy for 4 weeks. The size of lesion diminished 2.1 cm to 1.6 cm.
|
 | Fig. 4(A) Ultrasonography of patient in case 5 shows hypoechoic lesion about 2 cm sized. (B) We removed the lesion by mammotome, because the patient did not want surgery. She had recurrence after 9 months at the same position.
|
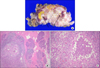 | Fig. 5(A) Gross photograph showing multiple purulent exudates. Arrow = focal inflammatory change. (B) Characteristic granulomatous inflammation is noted (H&E stain, ×40). (C) Granulomatous inflammation shows central inflammatory exudate and palisading epithelioid cell and multinucleated giant cells (H&E stain, ×100).
|
 | Fig. 6Postoperative photogram. This patient practiced quadrantectomy with reconstruction with pectoralis major muscle flap for treatment of idiopathic granulomatous mastitis.
|
Table 1
Clinicopathological overview of 14 cases with idiopathic granulomatous mastitis

*Cosmesis evaluated by excellent, good, fair and poor; †,‡The same patients who affected bilateral breast; §This case performed mammotome for excision of the breast lesion, but recurred the idiopathic granulomatous mastitis after 9 months. We treated this case with steroid therapy and surgically complete excision, who had no recurrence at 21 months; ∥Quadrantectomy and reconstruction with vicryl mesh; ¶Quadrantectomy and reconstruction with pectoralis major muscle flap.
![]()
References
1. Bani-Hani KE, Yaghan RJ, Matalka II, Shatnawi NJ. Idiopathic granulomatous mastitis: time to avoid unnecessary mastectomies. Breast J. 2004. 10:318–322.
2. Fletcher A, Magrath IM, Riddell RH, Talbot IC. Granulomatous mastitis: a report of seven cases. J Clin Pathol. 1982. 35:941–945.
3. Diesing D, Axt-Fliedner R, Hornung D, Weiss JM, Diedrich K, Friedrich M. Granulomatous mastitis. Arch Gynecol Obstet. 2004. 269:233–236.
4. Lee JH, Kim HA, Moon BI, Lee RA, Sung SH. Granulomatous mastitis. J Korean Surg Soc. 2007. 72:94–100.
5. Kim YJ, Choi YJ, Kim JY, Kim HJ, Park YS, Hong SW, et al. Clinicopathologic features of granulomatous mastitis. Korean J Pathol. 2005. 39:181–186.
6. Wilson JP, Massoll N, Marshall J, Foss RM, Copeland EM, Grobmyer SR. Idiopathic granulomatous mastitis: in search of a therapeutic paradigm. Am Surg. 2007. 73:798–802.
7. Ayeva-Derman M, Perrotin F, Lefrancq T, Roy F, Lansac J, Body G. Idiopathic granulomatous mastitis. Review of the literature illustrated by 4 cases. J Gynecol Obstet Biol Reprod (Paris). 1999. 28:800–807.
8. Newnham MS, Shirley SE, McDonald AH. Granulomatous lobular mastitis. A case report and review of the literature. West Indian Med J. 2001. 50:236–238.
9. Kessler E, Wolloch Y. Granulomatous mastitis: a lesion clinically simulating carcinoma. Am J Clin Pathol. 1972. 58:642–646.
10. Erhan Y, Veral A, Kara E, Ozdemir N, Kapkac M, Ozdedeli E, et al. A clinicopthologic study of a rare clinical entity mimicking breast carcinoma: idiopathic granulomatous mastitis. Breast. 2000. 9:52–56.
11. Lee SD, Park HL, Nam SJ, Ko YH, Ree HJ, Han BK, et al. Diagnosis and treatment of granulomatous mastitis: a study of 12 cases. J Korean Surg Soc. 2000. 58:487–493.
12. Memis A, Bilgen I, Ustun EE, Ozdemir N, Erhan Y, Kapkac M. Granulomatous mastitis: imaging findings with histopathologic correlation. Clin Radiol. 2002. 57:1001–1006.
13. Asoglu O, Ozmen V, Karanlik H, Tunaci M, Cabioglu N, Igci A, et al. Feasibility of surgical management in patients with granulomatous mastitis. Breast J. 2005. 11:108–114.
14. Tse GM, Poon CS, Ramachandram K, Ma TK, Pang LM, Law BK, et al. Granulomatous mastitis: a clinicopathological review of 26 cases. Pathology. 2004. 36:254–257.
15. DeHertogh DA, Rossof AH, Harris AA, Economou SG. Prednisone management of granulomatous mastitis. N Engl J Med. 1980. 303:799–800.
16. Katz U, Molad Y, Ablin J, Ben-David D, Paran D, Gutman M, et al. Chronic idiopathic granulomatous mastitis. Ann N Y Acad Sci. 2007. 1108:603–608.
17. Al-Khaffaf B, Knox F, Bundred NJ. Idiopathic granulomatous mastitis: a 25-year experience. J Am Coll Surg. 2008. 206:269–273.
18. Lai EC, Chan WC, Ma TK, Tang AP, Poon CS, Leong HT. The role of conservative treatment in idiopathic granulomatous mastitis. Breast J. 2005. 11:454–456.
19. Azlina AF, Ariza Z, Arni T, Hisham AN. Chronic granulomatous mastitis: diagnostic and therapeutic considerations. World J Surg. 2003. 27:515–518.
 XML Download
XML Download