

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Primary aortocaval fistula (ACF) is a rare complication of abdominal aortic aneurysm (AAA), occurring in only 4% of ruptured cases and less than 1% of all AAAs. The hemodynamic changes resulting from the major shunt caused by the ACF include a sudden increase in inferior vena caval pressure and volume with renal venous hypertension and a decrease in total peripheral resistance. So, if untreated, it leads to irreversible high output heart failure. Preoperative diagnosis is crucial, as adequate preparation should be made for massive bleeding expected at operation. Successful treatment depends on management of perioperative hemodynamics, control of bleeding from fistula and prevention of thromboembolism. We report two cases of successfully treated spontaneous ACF with a review of the literature.
Figures and Tables
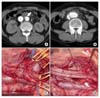 | Fig. 1Patient #1. (A) Early synchronous and equivalent enhancement of the IVC and aorta and localized intimal dissection of aorta (arrow). (B) 4 cm sized infrarenal abdominal aortic aneurysm. (C) Control of both iliac arteries and veins. (D) Dacron patch closure of fistula (arrow) and bifurcated graft.
|
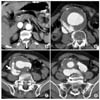 | Fig. 2Patient #2. CT findings of aortocaval fistula associated with abdominal aortic aneurysm (A) early synchronous and equivalent enhancement of the IVC and aorta (B) 9×8 cm sized infrarenal abdominal aortic aneurysm (C) direct visualization of aortocaval fistula (arrow) (D) both common iliac artery aneurysm.
|

References
1. Cooley DA. Resection of ruptured aneurysms of the abdominal aorta. Discussion of David M, Dyes WS, Grave IS, et al. Ann Surg. 1955. 142:623.
2. Brewster DC, Cambria RP, Moncure AC, Darling RC, LaMuraglia GM, Geller SC, et al. Aortocaval and iliac arteriovenous fistulas: recognition and treatment. J Vasc Surg. 1991. 13:253–265.
3. Javid H, Dye WS, Grove WJ, Julian OC. Resection of ruptured aneurysms of the abdominal aorta. Ann Surg. 1955. 142:613–621.
4. Bednarkiewicz M, Pretre R, Kalangos A, Khatchatourian G, Bruschweiler I, Faidutti B. Aortocaval fistula associated with abdominal aortic aneurysm: a diagnostic challenge. Ann Vasc Surg. 1997. 11:464–466.
5. Callogaro KD, Savarese RP, DeLaurentis DA. Unusual aspects of aortovenous fistulas associated with ruptured abdominal aortic aneurysms. J Vasc Surg. 1990. 12:586–590.
6. Gilling-Smith GL, Mansfield AO. Spontaneous abdominal arteriovenous fistulae: report of eight cases and review of the literature. Br J Surg. 1991. 78:421–425.
7. Coulier B, Tilquin O, Etienne PY. Multidetector row CT diagnosis of aortocaval fistula complicating aortic aneurysm: a case report. Emerg Radiol. 2004. 11:100–103.
8. Maeda H, Umezawa H, Goshima M, Hattori T, Nakamura T, Nishii T, et al. Surgery for ruptured abdominal aortic aneurysm with an aortocaval and iliac vein fistula. Surg Today. 2007. 37:445–448.
9. Lay JP, Swainson CJ, Sukumar SA. Paradoxical pulmonary embolism secondary to aortocaval fistula: diagnosis by helical CT. Br J Radiol. 1999. 72:507–509.
10. Vetrhus M, McWilliams R, Tan CK, Brennan J, Gilling-Smith G, Harris PL. Endovascular repair of abdominal aortic aneurysms with aortocaval fistula. Eur J Vasc Endovasc Surg. 2005. 30:640–643.
 XML Download
XML Download