

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hip joint is an unusual site in incidence for ganglion cysts, which are commonly located on wrist, ankle or knee.(1) Ganglion cysts on hip joint can compress the femoral vessels and cause ipsilateral leg swelling or claudication.(1,2) Only two cases with leg swelling by ganglion cysts were reported in medical literature in western countries but it has not been reported yet in Asia. We herein present a case of the left leg swelling due to the femoral vein compression by a ganglion cyst on hip joint.
CASE REPORT
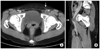
A 37-year-old woman was presented with gradually increasing swelling of the left lower leg that had been detected incidentally two months ago. She denied any history of trauma. There was no past medical history for deep vein thrombosis. The entire left leg was swollen but the foot was spared. Mass was not palpable in the inguinal area and there was no abnormality through the physical examination other than leg swelling. Left mid-thigh and mid-calf circumference was thicker than the right side by 7 cm and 3 cm, respectively. Deep vein thrombosis was suspected but the laboratory test was normal in DIC battery (FDP, d-Dimer) and other hypercoagulable factors (protein C/S, antiphospholipid antibody, lupus anticoagulant and antithrombin III). CT showed a 2.7 cm-sized relatively well circumscribed low attenuation mass with compressing the left common femoral vein (Fig. 1).
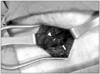
At operation, a 2.5 cm-sized cystic mass which consisted of thin walls and was full of jelly-like materials was compressing the femoral vein antero-medially (Fig. 2). It was communicated with the hip joint and easily dissected from the femoral vein. Surgical excision of the mass and ligation of the pedicle to the hip joint was done without venous reconstruction. Histologically, the cyst wall was composed of dense fibrous tissue and there was no synovial lining, which was compatible with a ganglion cyst. Patient discharged at three postoperative days without any complications. Swelling could be shrunk to normal size in a week. There was no evidence of recurrence and the femoral vein compression by a duplex ultrasound after six month follow-up.
DISCUSSION
Ganglion cysts are benign mass that arise from synovial membrane of joint or tendon sheath, and usually occur on wrist, knee or ankle. Though ganglion cysts can develop after trauma or be associated with arthritis, their pathogenesis has not been known clearly. Ganglion cysts have been considered to occur by outpouching of the joint capsule, embryologic remnant of synovial tissue, connective tissue degeneration by trauma or weakness of tissue by extensive joint movement.(1,3)
Joint related cysts can be divided largely into ganglion cysts and synovial cysts by their histological finding. Ganglion cysts have less synovial lining in capsule, more jelly-like contents and rare communication with the joint than synovial cysts. Despite histological differences, their prognosis and treatment are almost same. Leg swelling by cysts related to joint is very rare and only two cases, to our knowledge, were reported due to ganglion cysts in medical literature in western countries.(1) Adventitial cysts are another cause of the femoral vein compression, and their pathogenesis is thought to be identical with cystic degeneration of the popliteal artery. Ganglion cysts and adventitial cysts are identical in clinical and morphological Features. However, femoral vein injury can occur during surgery of adventitial cyst because no dissection plane exists.(4,5)
Ganglion cysts are usually asymptomatic and innocuous but they can compress any structure and develop symptoms as they enlarge. Ganglion cysts can cause leg swelling or intermittent claudication by compressing vessels.(1,2) Weakness and referred pain can occur by the femoral nerve compression by cysts.(6-8) Ganglion cysts are not easy to palpate in inguinal and hip area because of their anatomic location, however, initial presentation can be a palpable mass in inguinal lesion, resembling hernia.(9)
Due to advanced imaging technology, it became easier to diagnose ganglion cysts. Cystic contents in ganglion cysts is well established and easily diagnosed by ultrasonogram, CT scan and MRI.(10) We can evaluate cystic characteristics more accurately in MRI than CT by showing intermediate or high signal density in T2-weighted image and low signal density in T1-weighted image. Sagittal view of CT or MRI reveals the relationship between the ganglion cyst and the adjacent structure well. Nowadays, venogram and arthrogram are hardly ever done by their invasive nature.
Ganglion cysts can be treated by large-bore needle aspiration or surgical excision. Asymptomatic and incidental ganglion cysts may be left untreated. But, in case of leg swelling, the femoral vein compression should be relieved using any form of previously described therapy in order to prevent venous thrombosis by stasis.(7) Ganglion cysts can be decompressed by needle aspiration at outpatient clinic, but it is not easy because of their jelly-like contents and high recurrence rate. Surgical excision is the procedure of choice in symptomatic cases and considerate care must be taken to ligate the pedicle of the ganglion cyst originating from joint or tendon sheath to prevent recurrence when the pedicle is present. Venous flow is usually restored and swelling is relieved right after surgical excision.
In conclusion, we should consider a ganglion cyst on hip joint as a rare cause of unilateral leg swelling, mimicking symptom of a deep vein thrombosis and high index of suspicion is needed as in this case.
 XML Download
XML Download