

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Ultralow anterior resection and coloanal anastomosis (hand-sewn) has commonly been used for preserving the anal sphincter in patients with low-lying distal rectal cancer. Preoperative chemoradiation therapy is a contributing factor to preserve the anal sphincter. Intersphincteric resection has been introduced and has begun to be applied to distal rectal cancer for anal sphincter preservation. The aim of this study was to report on patients who underwent intersphincteric resection and coloanal anastomosis for very low-lying rectal cancer.
Methods
Intersphincteric resection was performed in 21 patients with very low-lying rectal cancer (within 4 cm from the anal verge) between December 2004 and May 2008. All patients received colonic J pouch anal anastomosis and loop ileostomy. The patients were selected prospectively and followed up for the function of bowel movement and recurrence.
Results
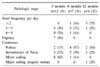
Mean tumor distance from anal verge was 2.8 cm (range 2~4 cm). No postoperative mortality was encountered. One patient developed ischemic colitis of colonic J-pouch after high doses of tomotherapy. Subsequently he received abdominoperineal resection and permanent colostomy. One patient underwent diverting colostomy for severe incontinence after ileostomy takedown. The other cases reported good anorectal function such as frequency of bowel movement and fecal incontinence. There were two local recurrences during a mean follow-up period of 11.6 months.
Figures and Tables
 | Fig. 1Scheme of intersphincteric resection for distal rectal cancer using concurrenct chemoradiotherapy. (a) Rectal tumor before chemoradiation presenting as an infiltrative lesion. (b) Rectal tumor after chemoradiation showing decreased tumor size. (c) Fibrotic change of previous tumor infiltrative lesion. (d) Surgical plane of intersphincteric resection allowing adequate distal margin. IS = internal anal sphincter; ES = external anal sphincter; PR = puborectalis; CRT = chemoradiation therapy.
|
 | Fig. 2Surgical technique of intersphincteric resection. (A) Circumferential incision of the anal mucosa. (B) Dissection of intersphincteric space between internal and external anal sphincter. (C) Hand-sewn anastomosis among colonic J pouch, external anal sphincter, and anoderm made at the level of dentate line.
|
 | Fig. 3Colonoscopic findings of rectal cancer before (A) and after (B) preoperative chemoradiotherapy. Ulcerofungating mass shrinked into small ulcerative lesion.
|
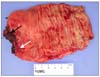 | Fig. 4Surgical specimen of intersphincteric resectioin. Previous tumor was changed to fibrous scar after preoperative chemoradiotherapy (white arrow). Internal sphincter was completely resected with the specimen (black arrow).
|


References
1. Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery-the clue to pelvic recurrence? Br J Surg. 1982. 69:613–616.
2. Chessin DB, Guillem JG. Surgical issues in rectal cancer: a 2004 update. Clin Colorectal Cancer. 2004. 4:233–240.
3. Jeong SY, Chessin DB, Guillem JG. Surgical treatment of rectal cancer: radical resection. Surg Oncol Clin N Am. 2006. 15:95–107.
4. Kim NK, Min BS, Kim JS, Hur H, Lee KY, Sohn SK, et al. Oncologic outcomes and safety after tumor-specific mesorectal excision for respectable rectal cancer: a single institution's experience with 1,276 patients with rectal cancer. J Korean Soc Coloproctol. 2008. 24:121–133.
5. Williams NS, Dixon MF, Johnston D. Reappraisal of the 5 centimetre rule of distal excision for carcinoma of the rectum: a study of distal intramural spread and of patients' survival. Br J Surg. 1983. 70:150–154.
6. Rullier E, Goffre B, Bonnel C, Zerbib F, Caudry M, Saric J. Preoperative radiochemotherapy and sphincter-saving resection for T3 carcinomas of the lower third of the rectum. Ann Surg. 2001. 234:633–640.
7. Schiessel R, Karner-Hanusch J, Herbst F, Teleky B, Wunderlich M. Intersphincteric resection for low rectal tumours. Br J Surg. 1994. 81:1376–1378.
8. Rullier E, Zerbib F, Laurent C, Bonnel C, Caudry M, Saric J, et al. Intersphincteric resection with excision of internal anal sphincter for conservative treatment of very low rectal cancer. Dis Colon Rectum. 1999. 42:1168–1175.
9. Saito N, Ono M, Sugito M, Ito M, Morihiro M, Kosugi C, et al. Early results of intersphincteric resection for patients with very low rectal cancer: an active approach to avoid a permanent colostomy. Dis Colon Rectum. 2004. 47:459–466.
10. Rullier E, Laurent C, Bretagnol F, Rullier A, Vendrely V, Zerbib F. Sphincter-saving resection for all rectal carcinomas: the end of the 2 cm distal rule. Ann Surg. 2005. 241:465–469.
11. Schiessel R, Novi G, Holzer B, Rosen HR, Renner K, Holbling N, et al. Technique and long-term results of intersphincteric resection for low rectal cancer. Dis Colon Rectum. 2005. 48:1858–1865.
12. Shirouzu K, Ogata Y, Araki Y, Kishimoto Y, Sato Y. A new ultimate anus-preserving operation for extremely low rectal cancer and for anal cancer. Tech Coloproctol. 2003. 7:203–206.
13. Kim JH, Oh NG. Intersphincteric resection for very low rectal cancer. J Korean Soc Coloproctol. 2004. 20:364–370.
14. Kim NK, Lim DJ, Yun SH, Sohn SK, Min JS. Ultralow anterior resection and coloanal anastomosis for distal rectal cancer: functional and oncological results. Int J Colorectal Dis. 2001. 16:234–237.
15. Saito N, Moriya Y, Shirouzu K, Maeda K, Mochizuki H, Koda K, et al. Intersphincteric resection in patients with very low rectal cancer: a review of the Japanese experience. Dis Colon Rectum. 2006. 49:S13–S22.
16. Urban M, Rosen HR, Holbling N, Feil W, Hochwarther G, Hruby W, et al. MR imaging for the preoperative planning of sphincter-saving surgery for tumors of the lower third of the rectum: use of intravenous and endorectal contrast materials. Radiology. 2000. 214:503–508.
17. Holzer B, Urban M, Holbling N, Feil W, Novi G, Hruby W, et al. Magnetic resonance imaging predicts sphincter invasion of low rectal cancer and influences selection of operation. Surgery. 2003. 133:656–661.
18. Bretagnol F, Rullier E, Laurent C, Zerbib F, Gontier R, Saric J. Comparison of functional results and quality of life between intersphincteric resection and conventional coloanal anastomosis for low rectal cancer. Dis Colon Rectum. 2004. 47:832–838.
19. Kohler A, Athanasiadis S, Ommer A, Psarakis E. Long-term results of low anterior resection with intersphincteric anastomosis in carcinoma of the lower one-third of the rectum: analysis of 31 patients. Dis Colon Rectum. 2000. 43:843–850.
 XML Download
XML Download