

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The lung represents the second most metastatic site after the liver in colorectal cancer (CRC). Traditionally, pulmonary metastasis has been evaluated by means of a chest X-ray. But, recently, chest computed tomography (CT) is increasingly being performed to detect pulmonary metastasis in CRC. This study was performed to evaluate the usefulness of chest CT over chest X-ray for early detection of pulmonary metastasis in preoperative staging in CRC.
Methods
We retrospectively reviewed 108 cases of CRC patients surgically treated with a curative intent at Chonbuk National University Hospital from April, 2007 to December, 2007. All evaluated by both chest X-ray and chest CT preoperatively.
Results
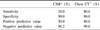
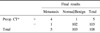
Five among 108 patients had metastatic lesions of the lung. Four of these 5 patients (80%) had a positive chest CT. But one of these 5 patients (20%) had a positive chest X-ray. Chest CT provided a sensitivity of 80% and a positive predictive value of 80% for the detection of metastatic lesions of the lung. In contrast, chest X-ray provided a sensitivity of 20% and a positive predictive value of 50% for the detection of metastatic lesion of the lung. Nine of these 108 patients (8%) were diagnosed with solitary pulmonary nodule (SPN) and one of them was confirmed to have metastatic lesion of the lung.
Figures and Tables
 | Fig. 1Undetected right lung mass on chest X-ray: mass in the right lung in a 64-year-old man with colon cancer. (A) This figure shows no evidence of the malignant lesion of the chest. (B) This figure shows malignant lesion of the subpleural lesion of the right lung.
|
 | Fig. 2Neglected right lung mass: increased size of the mass in the right lung in a 77-year-old man with colon cancer. (A) This figure shows a lesion in the right lung and was not believed to be metastatic disease. (B) Four months later, the size of the mass was increased.
|


References
1. McIntosh J, Sylvester PA, Virjee J, Callaway M, Thomas MG. Pulmonary staging in colorectal cancer--is computerised tomography the answer? Ann R Coll Surg Engl. 2005. 87:331–333.
2. Simo M, Lomena F, Setoain J, Perez G, Castellucci P, Costansa JM, et al. FDG-PET improves the management of patients with suspected recurrence of colorectal cancer. Nucl Med Commun. 2002. 23:975–982.
3. Engstrom PF, Arnoletti JP, Benson AB 3rd, Chen YJ, Choti MA, Cooper HS, et al. Colon cancer. J Natl Compr Canc Netw. 2007. 5:884–925.
4. Moore KH, McCaughan BC. Surgical resection for pulmonary metastases from colorectal cancer. ANZ J Surg. 2001. 71:143–146.
5. Inoue M, Kotake Y, Nakagawa K, Fujiwara K, Fukuhara K, Yasumitsu T. Surgery for pulmonary metastases from colorectal carcinoma. Ann Thorac Surg. 2000. 70:380–383.
6. Hatanaka K. CT evaluation of pulmonary metastases: usefulness in comparison with chest radiography. Nippon Igaku Hoshasen Gakkai Zasshi. 1999. 59:663–669.
7. Ike H, Shimada H, Ohki S, Togo S, Yamaguchi S, Ichikawa Y. Results of aggressive resection of lung metastases from colorectal carcinoma detected by intensive follow-up. Dis Colon Rectum. 2002. 45:468–473.
8. Schoemaker D, Black R, Giles L, Toouli J. Yearly colonoscopy, liver CT, and chest radiography do not influence 5-year survival of colorectal cancer patients. Gastroenterology. 1998. 114:7–14.
9. Rotolo N, De Monte L, Imperatori A, Dominioni L. Pulmonary resections of single metastases from colorectal cancer. Surg Oncol. 2007. 16:Suppl 1. S141–S144.
10. van Schaik PM, Kouwenhoven EA, Bolhuis RJ, Biesma B, Bosscha K. Pulmonary resection for metastases from colorectal cancer. J Thorac Oncol. 2007. 2:652–656.
11. Takahashi S, Nagai K, Saito N, Konishi M, Nakagohri T, Gotohda N, et al. Multiple resections for hepatic and pulmonary metastases of colorectal carcinoma. Jpn J Clin Oncol. 2007. 37:186–192.
12. Yedibela S, Klein P, Feuchter K, Hoffmann M, Meyer T, Papadopoulos T, et al. Surgical management of pulmonary metastases from colorectal cancer in 153 patients. Ann Surg Oncol. 2006. 13:1538–1544.
13. Wormanns D, Diederich S. Characterization of small pulmonary nodules by CT. Eur Radiol. 2004. 14:1380–1391.
14. Winer-Muram HT. The solitary pulmonary nodule. Radiology. 2006. 239:34–49.
15. Tan BB, Flaherty KR, Kazerooni EA, Iannettoni MD. The solitary pulmonary nodule. Chest. 2003. 123:89S–96S.
16. Jeong YJ, Yi CA, Lee KS. Solitary pulmonary nodules: detection, characterization, and guidance for further diagnostic workup and treatment. AJR Am J Roentgenol. 2007. 188:57–68.
17. Kim HJ. Current situation of tuberculosis and its control in Korea. J Korean Med Assoc. 2006. 49:762–772.
 XML Download
XML Download