

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the effect of endonasal dacryocystorhinostomy in the paranasal mucocele invading nasolacrimal duct.
Methods
We analyzed 252 patients who were diagnosed with paranasal mucocele from 2006 to 2017, and found 14 patients (14 eyes) who underwent endonasal dacryocystorhinostomy in the paranasal mucocele invading nasolacrimal duct. Clinical features and surgical results of the patients were analyzed retrospectively.
Results
The origins of the mucocele were frontoethmoidal sinus (seven cases, 50%) and ethmoidal sinus(seven cases, 50%). The most common symptom from the first visit was epiphora (13 cases, 92.8%); medial canthal mass (nine cases, 64.2%) was the second most common symptom. Every patient underwent endonasal dacryocystorhinostomy with rhinology and sinus surgery according to the type, size, and severity of the paranasal mucocele. Every patient showed successful irrigation in the lacrimal canalicular irrigation test and improved epiphora 6 months postoperatively.
Conclusions
When paranasal mucocele invades the orbit, it can cause diplopia, exophthalmos, extraocular muscle movement disorders, visual impairments, and increased intraocular pressure. Furthermore, if it invades the nasolacrimal duct, it can cause obstruction of the nasolacrimal duct and result in epiphora. Based on our results, endonasal dacryocystorhinostomy was an effective primary treatment.
Figures and Tables
 | Figure 1Computed tomography (CT) scan image of ethmoidal mucocele invading nasolacrimal duct (white arrow). (A) Axial view of CT scan images. (B) Coronal view of CT scan images.
|
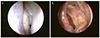 | Figure 2Intranasal endoscopic view of left nasal cavity. (A) Black arrow indicates ethmoidal mucocele. (B) Left nasal cavity at 6 months after the surgery. Mucocele was successfully removed and there were no signs of recurrence.
|




Notes
References
1. Beasley NJ, Jones NS. Paranasal sinus mucoceles: modern management. Am J Rhinol. 1995; 9:251–256.

2. Lund VJ, Harvey W, Meghji S, Harris M. Prostaglandin synthesis in the pathogenesis of fronto-ethmoidal mucoceles. Acta Otolaryngol. 1988; 106:145–151.
3. Haik BG, Amedee RG. Principles and practice of ophthalmic plastic and reconstructive surgery. 2nd ed. Philadelphia: WB Saunders;1996. p. 1014–1022. Vol. 2.
4. Evans C. Aetiology and treatment of fronto-ethmoidal mucocele. J Laryngol Otol. 1981; 95:361–375.
5. Moriyama H, Nakajima T, Honda Y. Studies on mucocoeles of the ethmoid and sphenoid sinuses: analysis of 47 cases. J Laryngol Otol. 1992; 106:23–27.
6. Tseng CC, Ho CY, Kao SC. Ophthalmic manifestations of paranasal sinus mucoceles. J Chin Med Assoc. 2005; 68:260–264.
7. Précausta F, Goga D, Laure B. Mucocèle ethmoïdale découverte devant un épiphora. J Fr Ophtalmol. 2013; 36:e169–e172.
8. Munk PL, Lin DT, Morris DC. Epiphora: treatment by means of dacryocystoplasty with balloon dilation of the nasolacrimal drainage apparatus. Radiology. 1990; 177:687–690.
9. Natvig K, Larsen TE. Mucocele of the paranasal sinuses. A retrospective clinical and histological study. J Laryngol Otol. 1978; 92:1075–1082.
10. East D. Mucocoeles of the maxillary antrum. Description, case reports and review of the literature. J Laryngol Otol. 1985; 99:49–56.
11. Kim SS, Kang SS, Kim KS, et al. Clinical characteristics of primary paranasal sinus mucoceles and their surgical treatment outcome. Korean J Otorhinolaryngol-Head Neck Surg. 1998; 41:1436–1439.
12. Kim JL, Yang JW. Clinical characteristics of paranasal sinus mucoceles which invade the orbit. J Korean Ophthalmol Soc. 2008; 49:562–569.
13. Barnes L. Surgical Pathology of the Head and Neck. 2nd ed. New York: CRC Press;2000. p. 445–469. Vol. 1.
14. Kennedy DW, Josephson JS, Zinreich SJ, et al. Endoscopic sinus surgery for mucoceles: a viable alternative. Laryngoscope. 1989; 99:885–895.
15. Shin HH, Lee TS, Baek SH. The comparision of surgical results of endonasal dacryocystorhinostomy in childen and adults. J Korean Ophthalmol Soc. 2006; 47:877–882.
 XML Download
XML Download