

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To determine the risk factors of intraoperative complications in femtosecond laser-assisted cataract surgery.
Methods
This study included 598 eyes of 337 patients who underwent femtosecond laser-assisted cataract surgery (FLACS) between July, 2012 and January, 2017. All eyes had corneal incisions, anterior capsulotomy, nuclear fragmentation, and limbal relaxing incisions (if required). Intraoperative complications were analyzed by watching videos, and the related factors of each complication were retrospectively reviewed alongside the medical records.
Results
The mean age of the patients was 62.1 ± 11.9 years. Among the study group, 18 eyes required manual creation of corneal incisions; because the corneal incisions could not be made due to corneal central opacity, corneal peripheral degeneration, ptreygium, conjunctival chalasis, or idiopathic. The anterior capsulotomy was incomplete in 43 cases and manual capsulorrhexis was required for completion. These cases were associated with various conditions, including hypermature cataract, anterior polar or subcapsular cataract, corneal central opacity, pupillary abnormality, lens subluxation, poor pupil dilation, and idiopathic. Overall, 22 eyes had difficulties with nuclear fragmentation, with either mature cataract, lens subluxation, corneal central opacity, anterior polar or subcapsular cataract, or pupillary abnormality. Using the Laser SoftFit™ patient interface decreased the incidences of incomplete corneal incision (from 3.56% to 2.24%, p = 0.367), anterior capsulotomy (from 9.31% to 4.03%, p < 0.05), and nuclear fragmentation (from 5.20% to 1.34%, p < 0.05). The incidences of complications in the experienced group was statistically lower compared with the novice group (p < 0.05 for all comparisons).
Conclusions
The femtosecond laser platform was effective and safe for cataract surgery. However, in the presence of related factors, use of this platform might need to be re-assessed and should be considered for intraoperative complications. Additionally, with the Laser SoftFit™ patient interface and improved surgeon experience, better intraoperative results can be expected for FLACS surgery.
Figures and Tables
 | Figure 1Advantages of SoftFit™ patient interface. In contrast to solid direct patient interface, the design of the new hydrogel SoftFit™ interface (white arrow) has an extended suction ring skirt that allows the natural curvature of the cornea and delivers a gentle, secure fit with minimal corneal distortion. With the soft contact lens in place, the intraocular pressure remains much lower during the procedure and corneal compression and corneal folds are minimized.
|
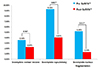 | Figure 2Rates of intraoperative complications before and after SoftFit™ interface. Comparison (%) of incomplete corneal incision, incomplete capsulotomy, incomplete nucleus fragmentation between femtosecond laser refractive cataract surgery with a direct contact interface (Pre-SoftFit™) and SoftFit™ interface (Post-SoftFit™). *p-value<0.05 between groups using Pearson Chi-square test.
|
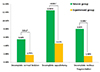 | Figure 3Rates of intraoperative complications between novice group and experienced group. Comparison (%) of incomplete corneal incision, incomplete capsulotomy, incomplete nucleus fragmentation between novice group (200 cases) and experienced group (398 cases). *p-value < 0.05 between groups using Pearson Chi-square test.
|

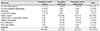
Table 2
List of intraoperative complications encountered in femtosecond laser cataract surgery cases (N = 598)

![]()


References
1. Krasnov MM. Laser-phakopuncture in the treatment of soft cataracts. Br J Ophthalmol. 1975; 59:96–98.
2. Ratkay-Traub I, Juhasz T, Horvath C, et al. Ultra-short pulse (femtosecond) laser surgery: initial use in LASIK flap creation. Ophthalmol Clin North Am. 2001; 14:347–355. viii–ix.
3. Sugar A. Ultrafast (femtosecond) laser refractive surgery. Curr Opin Ophthalmol. 2002; 13:246–249.
4. Nagy Z, Takacs A, Filkorn T, Sarayba M. Initial clinical evaluation of an intraocular femtosecond laser in cataract surgery. J Refract Surg. 2009; 25:1053–1060.
5. Masket S, Sarayba M, Ignacio T, Fram N. Femtosecond laser-assisted cataract incisions: architectural stability and reproducibility. J Cataract Refract Surg. 2010; 36:1048–1049.
6. Chang JS, Chen IN, Chan WM, et al. Initial evaluation of a femtosecond laser system in cataract surgery. J Cataract Refract Surg. 2014; 40:29–36.
7. Park JH, Lee KH, Lee DJ. Comparison of continuous curvilinear capsulorhexis parameters between femtosecond laser and conventional cataract surgery. J Korean Ophthalmol Soc. 2014; 55:1800–1807.
8. Kránitz K, Takacs A, Miháltz K, et al. Femtosecond laser capsulotomy and manual continuous curvilinear capsulorrhexis parameters and their effects on intraocular lens centration. J Refract Surg. 2011; 27:558–563.
9. Friedman NJ, Palanker DV, Schuele G, et al. Femtosecond laser capsulotomy. J Cataract Refract Surg. 2011; 37:1189–1198.
10. Auffarth GU, Reddy KP, Ritter R, et al. Comparison of the maximum applicable stretch force after femtosecond laser-assisted and manual anterior capsulotomy. J Cataract Refract Surg. 2013; 39:105–109.
11. Conrad-Hengerer I, Hengerer FH, Schultz T, Dick HB. Effect of femtosecond laser fragmentation on effective phacoemulsification time in cataract surgery. J Refract Surg. 2012; 28:879–883.
12. Conrad-Hengerer I, Hengerer FH, Schultz T, Dick HB. Effect of femtosecond laser fragmentation of the nucleus with different softening grid sizes on effective phaco time in cataract surgery. J Cataract Refract Surg. 2012; 38:1888–1894.
13. Abell RG, Kerr NM, Vote BJ. Toward zero effective phacoemulsification time using femtosecond laser pretreatment. Ophthalmology. 2013; 120:942–948.
14. Kránitz K, Miháltz K, Sándor GL, et al. Intraocular lens tilt and decentration measured by Scheimpflug camera following manual or femtosecond laser-created continuous circular capsulotomy. J Refract Surg. 2014; 28:259–263.
15. Miháltz K, Knorz MC, Alió JL, et al. Internal aberrations and optical quality after femtosecond laser anterior capsulotomy in cataract surgery. J Refract Surg. 2012; 27:711–716.
16. Takács AI, Kovács I, Miháltz K, et al. Central corneal volume and endothelial cell count following femtosecond laser-assisted refractive cataract surgery compared to conventional phacoemulsification. J Refract Surg. 2012; 28:387–391.
17. Conrad-Hengerer I, Al Juburi M, Schultz T, et al. Corneal endothelial cell loss and corneal thickness in conventional compared with femtosecond laser-assisted cataract surgery: three-month follow-up. J Cataract Refract Surg. 2013; 39:1307–1313.
18. Abell RG, Allen PL, Vote BJ. Anterior chamber flare after femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2013; 39:1321–1326.
19. Chen M. A review of femtosecond laser assisted cataract surgery for Hawaii. Hawaii J Med Public Health. 2013; 72:152–155.
20. Filkorn T, Kovács I, Takács A, et al. Comparison of IOL power calculation and refractive outcome after laser refractive cataract surgery with a femtosecond laser versus conventional phacoemulsification. J Refract Surg. 2012; 28:540–544.
21. Roberts TV, Lawless M, Bali SJ, et al. Surgical outcomes and safety of femtosecond laser cataract surgery: a prospective study of 1500 consecutive cases. Ophthalmology. 2013; 120:227–233.
22. Abell RG, Darian-Smith E, Kan JB, et al. Femtosecond laser-assisted cataract surgery versus standard phacoemulsification cataract surgery: outcomes and safety in more than 4000 cases at a single center. J Cataract Refract Surg. 2015; 41:47–52.
23. Chen M, Swinney C, Chen M. Comparing the intraoperative complication rate of femtosecond laser-assisted cataract surgery to traditional phacoemulsification. Int J Ophthalmol. 2015; 8:201–203.
24. Asena BS, Kaskaloglu M. Laser-assisted cataract surgery: soft lens assisted interface (SoftFit) versus direct contact interface. Eur J Ophthalmol. 2016; 26:242–247.
25. Chee SP, Yang Y, Ti SE. Clinical outcomes in the first two years of femtosecond laser-assisted cataract surgery. Am J Ophthalmol. 2015; 159:714–719.
26. Bali SJ, Hodge C, Lawless M, et al. Early experience with the femtosecond laser for cataract surgery. Ophthalmology. 2012; 119:891–899.
 XML Download
XML Download