

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To report a case of delayed infective endophthalmitis associated with exposure of scleral fixation knot.
Case summary
A 35-year-old female was transferred from a local clinic with sudden onset right eye pain under suspicion of uveitis. The patient received vitrectomy, scleral encircling and lensectomy for rhegmatogenous retinal detachment before 16 years. In addition, she underwent secondary scleral fixation of intraocular lens (IOL) 1 year previously. Best-corrected visual acuity was hand motion and intraocular pressure was 28 mmHg. Slit lamp examination revealed diffuse keratic precipitates and anterior chamber reaction was 4 positive. Exposed scleral fixation knot outside conjunctiva at 2 o' clock combined with suppurative discharge was observed. On fundus examination, red reflex was decreased due to vitreous haze. She was diagnosed as infective endophthalmitis associated with exposure of scleral fixation knot. The patient received vitrectomy and intravitreal injection of antibiotics and vitreous culture. After 2 days, IOL removal, silicone oil tamponade and intravitreal injection of antibiotics were performed due to uncontrolled inflammation with accompanying hypopyon. Hemophilus influenza was isolated in the vitreous sample. Removal of silicone oil was performed at 1 month. There was no recurrent inflammation at 1 year and she received scleral fixation of IOL for the second time. At 1 year and 3 months, corrected visual acuity was 0.4 without signs of inflammation.
Figures and Tables
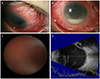
Figure 1
Preoperative clinical findings. (A) The photograph about exposure of the end of a scleral fixation suture through the conjunctiva at two o' clock on the right eye (arrow). (B) Keratic precipitates, hypopyon and severe conjunctival injection. (C) Blurry fundus due to severe vitritis. (D) Classic appearance of vitreous opacities, vitreous strands and membrane on B-scan ultrasonography.

References
1. Baykara M. Suture burial technique in scleral fixation. J Cataract Refract Surg. 2004; 30:957–959.
2. Malbran ES, Malbran E Jr, Negri I. Lens quide suture for transport and fixation in secondary IOL implantation after intracapsular extraction. Int Ophthalmol. 1986; 9:151–160.
3. Oh HS, Chu YK, Kwon OW. Surgical technique for suture fixation of a single-piece hydrophilic acrylic intraocular lens in the absence of capsule support. J Cataract Refract Surg. 2007; 33:962–965.
4. Solomon K, Gussler JR, Gussler C, Van Meter WS. Incidence and management of complications of transsclerally sutured posterior chamber lenses. J Cataract Refract Surg. 1993; 19:488–493.
5. Scharioth GB, Prasad S, Georgalas I, et al. Intermediate results of sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg. 2010; 36:254–259.
6. Agarwal A, Kumar DA, Jacob S, et al. Fibrin glue-assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refract Surg. 2008; 34:1433–1438.
7. Ozmen AT, Dogru M, Erturk H, Ozcetin H. Transsclerally fixated intraocular lenses in children. Ophthalmic Surg Lasers. 2002; 33:394–399.
8. Koytak A, Sari ES, Altinisik M. Scleral fixation underneath an intact conjunctiva. J Refract Surg. 2013; 29:220–223.
9. Eifrig CW, Flynn HW Jr, Scott IU, Newton J. Acute-onset postoperative endophthalmitis: review of incidence and visual outcomes (1995-2001). Ophthalmic Surg Lasers. 2002; 33:373–378.
10. Everekiloglu C, Er H, Bekir NA, et al. Comparison of secondary implantation of flexible open-loop anterior chamber and scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg. 2003; 29:301–308.
11. Schechter RJ. Suture-wick endophthalmitis with sutured posterior chamber intraocular lenses. J Cataract Refract Surg. 1990; 16:755–756.
12. Heilskov T, Joondeph BC, Olsen KR, Blankenship GW. Late endophthalmitis after transscleral fixation of a posterior chamber intraocular lens. Arch Ophthalmol. 1989; 107:1427.
13. Yoder DM, Scott IU, Flynn HW Jr, Miller D. Endophthalmitis caused by Haemophilus influenzae. Ophthalmology. 2004; 111:2023–2026.
14. Mandelbaum S, Forster RK, Gelender H, Culbertson W. Late onset endophthalmitis associated with filtering blebs. Ophthalmology. 1985; 92:964–972.
15. Postlethwait RW. Long-term comparative study of nonabsorbable sutures. Ann Surg. 1970; 171:892–898.
16. Jung MO, Koh JW. Clinical results of modified ab externo and one-knot technique. J Korean Ophthalmol Soc. 2012; 53:1783–1788.
17. Szurman P, Petermeier K, Aisenbrey S, et al. Z-suture: a new knotless technique for transscleral suture fixation of intraocular implants. Br J Ophthalmol. 2010; 94:167–169.
18. Ma DJ, Kim MK, Wee WR. Knotless external fixation technique for posterior chamber intraocular lens transscleral fixation: A 5-case analysis. J Korean Ophthalmol Soc. 2012; 53:1609–1614.
19. Hu XT, Zhang ZD, Zhou R, Pan QT. Cauterization technique for suture erosion in transscleral fixation of intraocular lenses. Int J Ophthalmol. 2013; 6:892–894.
 XML Download
XML Download