

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To compare the effectiveness of toric intraocular lens (IOL) implantation and monofocal IOL implantation with a limbal relaxing incision (LRI) for correcting astigmatism in the Korean population.
Methods
The medical records of 79 patients (100 eyes) with corneal astigmatism over 1.25 diopters (D) who underwent toric IOL implantation (toric group; 54 eyes), monofocal IOL implantation with a concurrent LRI (LRI group; 24 eyes), or monofocal IOL implantation without correcting astigmatism (control group; 22 eyes), were retrospectively reviewed. For subgroup analyses, the three groups were subdivided according to preoperative astigmatic severity under 2.5 D. Visual, refractive, and keratometric outcomes were compared 2 and 6 months postoperatively.
Results
The uncorrected distance visual acuity was at least 20/25 (0.1 logMAR) in 64.8%, 41.7%, and 27.3% of the toric, LRI, and control group eyes, respectively at 2 months after surgery. The toric group had the greatest refractive cylindrical error change (toric group, −2.48 ± 1.84 D to −0.98 ± 0.92 D; LRI group, −2.02 ± 1.03 D to −1.65 ± 0.86 D; control group, −1.69 ± 0.88 D to −1.49 ± 0.60 D; p < 0.001) and the LRI group showed the greatest mean corneal cylindrical error change (toric group, 2.40 ± 1.33 D to 2.23 ± 1.42 D; LRI group, 1.86 ± 0.44 D to 1.29 ± 0.55 D; control group, 1.60 ± 0.39 D to 1.35 ± 0.60 D; p = 0.025). The 85 eyes with moderate corneal astigmatism (between 1.25 D and 2.5 D) were under evaluation. The toric group showed the highest mean refractive cylindrical change (0.97 ± 0.66 D; p < 0.001), followed by the LRI group (0.53 ± 0.87 D; p = 0.046).
Conclusions
Both surgical techniques significantly reduced astigmatism and had comparable visual outcomes. Toric IOL implantation was more reliable for correcting astigmatism than monofocal IOL implantation with a concurrent LRI regardless of the preoperative astigmatic severity. Both procedures were effective in reducing astigmatism in eyes with moderate corneal astigmatism.
Figures and Tables
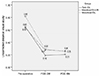 | Figure 1Pre- and postoperative uncorrected distance visual acuity of treatment groups (logMAR). All group showed significant improvement in uncorrected visual acuity. Toric IOL group showed the most difference compared to the other group. POD = postoperative day; M = months; IOL = intraocular lens; LRI = limbal relaxing incision.
|
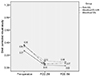 | Figure 2Pre- and postoperative best corrected visual acuity of treatment groups (logMAR). All group showed significant improvement in best corrected visual acuity. POD = postoperative day; M = months; IOL = intraocular lens; LRI = limbal relaxing incision.
|
 | Figure 3Pre- and postoperative cylindrical change of treatment groups (n = 100). Positive values represent keratometric astigmatism of each group, and negative values are refractive cylinder. POD = postoperative day; mo = months; IOL = intraocular lens; LRI = limbal relaxing incision.
|
 | Figure 4Scatter plots of the J0 and J45 vectors (in diopters [D]), calculated by power vector analysis of (A) toric IOL group, (B) LRI group, and (C) control groups. Black diamonds and gray squares indicate preoperative values and 2-months postoperative values, respectively. Preop = preoperative; Postop = postoperative; IOL = intraocular lens; LRI = limbal relaxing incision.
|
 | Figure 5Pre- and postoperative cylindrical change of treatment groups with keratometric astigmastism under 2.5 D (n = 85). Positive values represent keratometric astigmatism of each group, and negative values are refractive cylinder. POD = postoperative day; mo = months; IOL = intraocular lens; LRI = limbal relaxing incision.
|
Table 1
Preoperative demographic and biometric data of the subjects (n = 100)
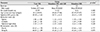
Values are presented as mean ± standard deviation unless otherwise indicated.
IOL = intraocular lens; LRI = limbal relaxing incision; D = diopters.
*One-way analysis of variance (ANOVA) test for age, Flat K, Steep K and Kruskall Wallis test for spherical IOL power, sphere, cylinder, spherical equivalent, each analyzing method used according to data normality.
![]()


References
1. Hoffer KJ. Biometry of 7,500 cataractous eyes. Am J Ophthalmol. 1980; 90:360–368.
2. Mohammad-Rabei H, Mohammad-Rabei E, Espandar G, et al. Three methods for correction of astigmatism during phacoemulsification. J Ophthalmic Vis Res. 2016; 11:162–167.
3. Steinert R. Cataract Surgery: Technique, Complications, and Management. 2nd ed. Philadelphia: Saunders;2003. p. 372.
4. Carvalho MJ, Suzuki SH, Freitas LL, et al. Limbal relaxing incisions to correct corneal astigmatism during phacoemulsification. J Refract Surg. 2007; 23:499–504.
5. Zare MA, Tehrani MH, Gohari M, et al. Management of corneal astigmatism by limbal relaxing incisions during cataract surgery. Iran J Ophthalmol. 2010; 22:15–20.
6. Budak K, Friedman NJ, Koch DD. Limbal relaxing incisions with cataract surgery. J Cataract Refract Surg. 1998; 24:503–508.
7. Yang SW, Lee JH, Lim SA, Chung SH. Comparison of the clinical outcomes of two types of toric intraocular lens. J Korean Ophthalmol Soc. 2016; 57:200–207.
8. Ahmed II, Rocha G, Slomovic AR, et al. Visual function and patient experience after bilateral implantation of toric intraocular lenses. J Cataract Refract Surg. 2010; 36:609–616.
9. Bauer NJ, de Vries NE, Webers CA, et al. Astigmatism management in cataract surgery with the AcrySof toric intraocular lens. J Cataract Refract Surg. 2008; 34:1483–1488.
10. De Silva DJ, Ramkissoon YD, Bloom PA. Evaluation of a toric intraocular lens with a Z-haptic. J Cataract Refract Surg. 2006; 32:1492–1498.
11. Entabi M, Harman F, Lee N, Bloom PA. Injectable 1-piece hydrophilic acrylic toric intraocular lens for cataract surgery: efficacy and stability. J Cataract Refract Surg. 2011; 37:235–240.
12. Mendicute J, Irigoyen C, Aramberri J, et al. Foldable toric intraocular lens for astigmatism correction in cataract patients. J Cataract Refract Surg. 2008; 34:601–607.
13. Poll JT, Wang L, Koch DD, Weikert MP. Correction of astigmatism during cataract surgery: toric intraocular lens compared to peripheral corneal relaxing incisions. J Refract Surg. 2011; 27:165–171.
14. Till JS, Yoder PR Jr, Wilcox TK, Spielman JL. Toric intraocular lens implantation: 100 consecutive cases. J Cataract Refract Surg. 2002; 28:295–301.
15. Nichamin LD. Management of astigmatism in conjunction with clear corneal phaco surgery. In : Gills JP, editor. A Complete Surgical Guide for Correcting Astigmatism: An Ophthalmic Manifesto. 1st ed. Thorofare: Slack, Inc.;2003. p. 41–47.
16. Na JH, Lee HS, Joo CK. The clinical result of AcrySof toric intraocular lens implantation. J Korean Ophthalmol Soc. 2009; 50:831–838.
17. Kawahara A, Takayanagi Y. Vector analysis investigation of toric intraocular lens with no deviation from the intended axis. Clin Ophthalmol. 2016; 10:2199–2203. eCollection 2016.
18. Ferreira TB, Almeida A. Comparison of the visual outcomes and OPD-scan results of AMO Tecnis toric and Alcon Acrysof IQ toric intraocular lenses. J Refract Surg. 2012; 28:551–555.
19. Miyata K, Miyai T, Minami K, et al. Limbal relaxing incisions using a reference point and corneal topography for intraoperative identification of the steepest meridian. J Refract Surg. 2011; 27:339–344.
20. Cha YJ, Kim MK, Wee WR. Effect of toric intraocular lens implantation on astigmatism in cataract surgery. J Korean Ophthalmol Soc. 2015; 56:1544–1551.
21. Ouchi M. High-cylinder toric intraocular lens implantation versus combined surgery of low-cylinder intraocular lens implantation and limbal relaxing incision for high-astigmatism eyes. Clin Ophthalmol. 2014; 8:661–667.
22. Budak K, Yilmaz G, Aslan BS, Duman S. Limbal relaxing incisions in congenital astigmatism: 6 month follow-up. J Cataract Refract Surg. 2001; 27:715–719.
23. Lee J, Lee H, Kang DS, et al. Comparison of toric foldable iris-fixated phakic intraocular lens implantation and limbal relaxing incisions for moderate-to-high myopic astigmatism. Yonsei Med J. 2016; 57:1475–1481.
24. Lam DK, Chow VW, Ye C, et al. Comparative evaluation of aspheric toric intraocular lens implantation and limbal relaxing incisions in eyes with cataracts and ≤3 dioptres of astigmatism. Br J Ophthalmol. 2016; 100:258–262.
 XML Download
XML Download