

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Case summary
A 69-year-old male patient was referred to the ophthalmologist from an otorhinolaryngology clinic due to mass invasion of the orbit on computed tomography. The patient had a history of ameloblastoma of the left maxilla, which had been diagnosed in 1988, and for which he had undergone left maxillectomy. He was transferred from a private hospital because of suspected tumor after frequent epistaxis at the left nasal cavity of about 1 year. The biopsy report confirmed that the mass was a recurrence of the ameloblastoma, and a 17.4 × 22.7 × 23.5-mm-sized mass that filled the left ethmoid sinus and invaded the nasal side of the orbit was found on paranasal sinus magnetic resonance imaging. There was no limitation of eye movement in any field of gaze in the left eye even though the patient reported diplopia. After maximum resection of the tumor using a debrider with endoscope, the size of the tumor was reduced and the symptom of diplopia was resolved. The patient will undergo continuous follow-up.
Figures and Tables
Figure 1
Clinical photograph on the first visit. It shows inferior displacement of left orbit due to previous left maxillectomy.

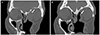
Figure 2
Well defined mass from left ethmoid sinus to medial orbit wall on magnetic resonance (MR) images. The mass shows low signal intensity on T1-weighted image (A, B) and high signal intensity on T2-weighted image (C, D) (arrow).

Figure 3
Histopathologic findings. The biopsy specimen shows plexiform pattern blanding ameloblastic cells arranged in anastomosing strands (Hematoxylin and eosin [HE] stain, ×200, HE stain, ×400) (A, B) (arrow). Immunohistopathology staining shows all negative result in CK7, CK20, CD117 and alpha smooth muscle actin (SMA) (C-F).

Notes
References
1. Garrity JA, Henderson JW, Cameron JD. Henderson's Orbital Tumors. 4th ed. Philadelphia: Lippincott Williams & Wilkins;2007. p. 81–121.
2. Cusack JW. Report of the amputations of the lower jaw. Dubliln Hop Rec. 1827; 4:1–38.
3. Kyriazis AP, Karkazis GC, Kyriazis AA. Maxillary ameloblastoma with intracerebral extension. Report of a case. Oral Surg Oral Med Oral Pathol. 1971; 32:582–587.
4. Iordanidis S, Makos C, Dimitrakopoulos J, Kariki H. Ameloblastoma of the maxilla. Case report. Aust Dent J. 1999; 44:51–55.
5. Weissman JL, Snyderman CH, Yousem SA, Curtin HD. Ameloblastoma of the maxilla: CT and MR appearance. AJNR Am J Neuroradiol. 1993; 14:223–226.
6. Weiss JS, Bressler SB, Jacobs EF Jr, et al. Maxillary ameloblastoma with orbital invasion. A clinicopathologic study. Ophthalmology. 1985; 92:710–713.
7. Leibovitch I, Schwarcz RM, Modjtahedi S, et al. Orbital invasion by recurrent maxillary ameloblastoma. Ophthalmology. 2006; 113:1227–1230.
8. Moon YI, Ahn S. A case report of ameloblastoma on left maxilla. Korean J Otorhinolaryngol-Head Neck Surg. 1980; 23:424–428.
9. Jang HS. A case report of recurred ameloblastoma. J Korean Assoc Oral Maxillofac Surg. 1996; 22:744–751.
10. Daramola JO, Abioye AA, Ajagbe HA, Aghadiuno PU. Maxillary malignant ameloblastoma with intra-orbital extension: report of case. J Oral Surg. 1980; 38:203–206.
11. Hayashi N, Iwata J, Masaoka N, et al. Ameloblastoma of the mandible metastasizing to the orbit with malignant transformation. A histopathological and immunohistochemical study. Virchows Arch. 1997; 430:501–507.
12. Bredenkamp JK, Zimmerman MC, Mickel RA. Maxillary ameloblastoma. A potentially lethal neoplasm. Arch Otolaryngol Head Neck Surg. 1989; 115:99–104.
13. Nastri AL, Wiesenfeld D, Radden BG, et al. Maxillary ameloblastoma: a retrospective study of 13 cases. Br J Oral Maxillofac Surg. 1995; 33:28–32.
14. Milman T, Lee V, LiVolsi V. Maxillary ameloblastoma with orbital involvement: An institutional experience and literature review. Ophthal Plast Reconstr Surg. 2016; 32:441–446.
15. Vaishampayan SS, Nair D, Patil A, Chaturvedi P. Recurrent ameloblastoma in temporal fossa: A diagnostic dilemma. Contemp Clin Dent. 2013; 4:220–222.
16. McClary AC, West RB, McClary AC, et al. Ameloblastoma: a clinical review and trends in management. Eur Arch Otorhinolaryngol. 2016; 273:1649–1661.
 XML Download
XML Download