

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the effects of anterior capsulotomy extension on the rotational stability of four different types of intraocular lenses (IOLs) and to analyze factors influencing IOL rotation.
Methods
The present single-center prospective study was comprised of 128 cataract patients (151 eyes) who underwent cataract surgery and received AcrySof IQ SN60WF, Tecnis ZA9003, Akreos MI60, or Zeiss XL Stabi ZO from March 2010 to December 2010. Sixty-four eyes received an anterior capsulotomy extension which was unintentionally created or performed using Vannas scissors after capsulorrhexis to prevent anterior capsular contracture. After pupil dilation, a digital retroillumination image of the IOL was taken on the operative day and 7 days postoperatively.
Results
There was no statistically significant difference in IOL rotation between the 4 types of IOL (p > 0.05). The anterior capsulotomy extension group (2.72 ± 2.42°) and the non-extension group (3.24 ± 2.16°) did not show statistically significant differences in IOL rotation (p > 0.05). A positive correlation was observed between age and IOL rotation. Axial length, anterior chamber depth, and anterior chamber volume did not affect the degree of rotation.
Conclusions
Among the 4 types of IOLs, there was no significant difference in rotational stability. Anterior capsulotomy extension to prevent anterior capsular contracture is not likely to significantly affect the rotational stability of IOLs; the 4 different types of IOL were stable in the eye and suitable as toric IOLs for correction of astigmatism.
Figures and Tables
Figure 1
Capsulotomy extension was performed using Vannas-scissor after capsulorrhexis. The yellow arrow indicated the 1-1.5 mm extending tear (XL Stabi ZO; Carl Zeiss Meditec SAS).
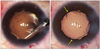
Figure 2
After confirmed maximum pupil dilation, photography of the IOL was taken directly at postoperative 1 day. Three reference axis were determined by taking 3 critical details; the optic center of the IOL, insertion of the haptics and one of the conjunctival vessels, episcleral vessels, or iris marking (SN60WF; Alcon).
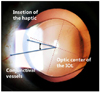
Figure 3
Mean postoperative IOL rotation degrees between 4 types of IOL. *p-value: statistical significance was calculated by oneway-ANOVA.
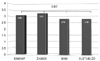
Figure 4
Comparison of mean postoperative IOL rotation degrees between non-extension group and extension group. *p-value: statistical significance was calculated by independent t-test; †p-value: statistical significance was calculated by Mann-Whitney U-test.

Figure 5
Comparison of mean postoperative IOL rotation degrees between other factors -haptic types, optic-haptic angulation, viscoelastics, and IOL design. *p-value: statistical significance was calculated by independent t-test.
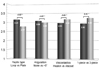
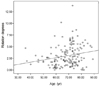
Figure 6
The scatterplots for mean difference of postoperative IOL rotation between age and postoperative rotation degrees (at 1 week after operation, r = 0.209, p < 0.05).



References
1. Hoffer KJ. Steinert RF, Howard Fine I, editors. The evolution of the intraocular lens. Cataract Surgery. 2004. 2nd ed. Philadelphia: Saunders;chap. 33.
2. Hoffer KJ. Biometry of 7,500 cataractous eyes. Am J Ophthalmol. 1980. 90:360–368.
3. Shin JW, Chung SK, Baek NH. The changes in the area of the anterior capsulotomy size. J Korean Ophthalmol Soc. 2001. 42:972–976.
4. Choi BJ, Hur J. Postoperative changes of continuous curvilinear capsulorhexis. J Korean Ophthalmol Soc. 1998. 39:1153–1158.
5. Na JH, Lee HS, Joo CK. The clinical result of AcrySof toric intraocular lens implantation. J Korean Ophthalmol Soc. 2009. 50:831–838.
6. Montés-Micó R, Cerviño A, Ferrer-Blasco T. Intraocular lens centration and stability: efficacy of current technique and technology. Curr Opin Ophthalmol. 2009. 20:33–36.
7. Entabi M, Harman F, Lee N, Bloom PA. Injectable 1-piece hydrophilic acrylic toric intraocular lens for cataract surgery: efficacy and stability. J Cataract Refract Surg. 2011. 37:235–240.
8. Buckhurst PJ, Wolffsohn JS, Naroo SA, Davies LN. Rotational and centration stability of an aspheric intraocular lens with a simulated toric design. J Cataract Refract Surg. 2010. 36:1523–1528.
9. Prinz A, Neumayer T, Buehl W, et al. Rotational stability and posterior capsule opacification of a plate-haptic and an open-loop-haptic intraocular lens. J Cataract Refract Surg. 2011. 37:251–257.
10. Novis C. Astigmatism and toric intraocular lenses. Curr Opin Ophthalmol. 2000. 11:47–50.
11. Viestenz A, Seitz B, Langenbucher A. Evaluating the eye's rotational stability during standard photography: effect on determining the axial orientation of toric intraocular lenses. J Cataract Refract Surg. 2005. 31:557–561.
12. Sun XY, Vicary D, Montgomery P, Griffiths M. Toric intraocular lenses for correcting astigmatism in 130 eyes. Ophthalmology. 2000. 107:1776–1781.
13. Till JS, Yoder PR Jr, Wilcox TK, Spielman JL. Toric intraocular lens implantation: 100 consecutive cases. J Cataract Refract Surg. 2002. 28:295–301.
14. Weinand F, Jung A, Stein A, et al. Rotational stability of a single-piece hydrophobic acrylic intraocular lens: new method for high-precision rotation control. J Cataract Refract Surg. 2007. 33:800–803.
15. Zuberbuhler B, Signer T, Gale R, Haefliger E. Rotational stability of the AcrySof SA60TT toric intraocular lenses: a cohort study. BMC Ophthalmol. 2008. 8:8.
16. Holland E, Lane S, Horn JD, et al. The AcrySof Toric intraocular lens in subjects with cataracts and corneal astigmatism: a randomized, subject-masked, parallel-group, 1-year study. Ophthalmology. 2010. 117:2104–2111.
17. Saldanha MJ, Benjamin L, Patel CK. Postoperative rotation of a 3-piece loop-haptic acrylic intraocular lens. J Cataract Refract Surg. 2009. 35:1751–1755.
18. Mendicute J, Irigoyen C, Aramberri J, et al. Foldable toric intraocular lens for astigmatism correction in cataract patients. J Cataract Refract Surg. 2008. 34:601–607.
19. Lane SS, Burgi P, Milios GS, et al. Comparison of the biomechanical behavior of foldable intraocular lenses. J Cataract Refract Surg. 2004. 30:2397–2402.
20. Koshy JJ, Nishi Y, Hirnschall N, et al. Rotational stability of a single-piece toric acrylic intraocular lens. J Cataract Refract Surg. 2010. 36:1665–1670.
21. Hayashi K, Hayashi H. Comparison of the stability of 1-piece and 3-piece acrylic intraocular lenses in the lens capsule. J Cataract Refract Surg. 2005. 31:337–342.
22. Chang DF. Early rotational stability of the longer Staar toric intraocular lens: fifty consecutive cases. J Cataract Refract Surg. 2003. 29:935–940.
23. Wolffsohn JS, Buckhurst PJ. Objective analysis of toric intraocular lens rotation and centration. J Cataract Refract Surg. 2010. 36:778–782.
24. Shah GD, Praveen MR, Vasavada AR, et al. Software-based assessment of postoperative rotation of toric intraocular lens. J Cataract Refract Surg. 2009. 35:413–418.
25. Nagata M, Matsushima H, Mukai K, et al. Comparison of anterior capsule contraction between 5 foldable intraocular lens models. J Cataract Refract Surg. 2008. 34:1495–1498.
26. Kwartz J, Edwards K. Evaluation of the long-term rotational stability of single-piece, acrylic intraocular lenses. Br J Ophthalmol. 2010. 94:1003–1006.
27. Patel CK, Ormonde S, Rosen PH, Bron AJ. Postoperative intraocular lens rotation: a randomized comparison of plate and loop haptic implants. Ophthalmology. 1999. 106:2190–2195.
 XML Download
XML Download