

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Case summary
A 43-year-old woman with no systemic disease complained of sudden inferior field defect of the right eye. On fundoscopic examination of the right eye, a single soft white spot was observed in the superotemporal vascular arcade. An elevated hyper-reflective area in the inner retina corresponding to a white spot was observed on optical coherence tomography. Automated perimetry revealed an arcuate field defect which was wider than the cotton-wool spot. A complete workup for systemic diseases was within normal range except a positive rheumatoid factor. At the 2-week follow-up, the patient's subjective symptom improved and the white spot decreased. After 6 months, the cotton-wool spot disappeared and slit-like retinal nerve fiber layer (RNFL) defects corresponding to the location of the cotton-wool spot was noticed. One year later, disc and RNFL defect were unchanged but the previous field defect disappeared.
Figures and Tables
 | Figure 1Initial fundus photographs showed the cotton wool spot in the right eye (A) and localized slit-like retinal nerve fiber layer (RNFL) defects in the left eye (B). RNFL thickness analysis by SD-OCT showed normal range of mean RNFL thickness in both eyes but deflection of RNFL thickness curve at the superior temporal area corresponding to the localized RNFL defect in the left eye was noticed (red circle). Static automated perimetry (SAP) of the right eye at the initial visit showed a focal defect which was located posterior to the location of cotton wool spot (orange circle) and the SAP of left eye was within normal limits.
|
 | Figure 2Fluorescein angiography at the initial visit. In early phase, focal filling defect in the region of the cotton wool spot was seen and mild hyperfluorescence surrounding the cotton wool spot appeared as time went.
|
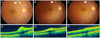 | Figure 3Serial fundus photographs and optical coherence tomography (OCT) scans taken at the initial visit, 1 month and 1 year later. A single white spot was seen in the temporal superior arcade (arrow) of the right eye (A). Fundus photograph 1 month later (B) showed a reduced cotton wool spot (arrow). One year later, the spot disappeared and localized slit-like retinal nerve fiber layer defect which did not reach the disc margin was noticed instead (C). OCT linear scan transversing the cotton wool spot showed elevated hyper-reflective area in the inner retina (D). But 1 month later, decreased hyper-reflective area in the inner retina was noticed (E). The smaller hyper-reflective area in the inner retina was seen, indicative of inner retinal gliosis but almost normal retinal structure was restored 1 year later (F).
|
References
1. Kozak I, Bartsch DU, Cheng L, Freeman WR. In vivo histology of cotton-wool spots using high-resolution optical coherence tomography. Am J Ophthalmol. 2006. 141:748–750.
2. Mansour AM, Jampol LM, Logani S, et al. Cotton-wool spots in acquired immunodeficiency syndrome compared with diabetes mellitus, systemic hypertension, and central retinal vein occlusion. Arch Ophthalmol. 1988. 106:1074–1077.
3. Remky A, Arend O. Single isolated cotton-wool spots. Ophthalmologica. 2000. 214:143–148.
4. McLeod D. Why cotton wool spots should not be regarded as retinal nerve fiber layer infarcts. Br J Ophthalmol. 2005. 89:229–237.
5. Shami MJ, Uy RN. Isolated cotton-wool spots in a 67-year-old woman. Surv Ophthalmol. 1996. 40:413–415.
6. Brown GC, Brown MM, Hiller T, et al. Cotton-wool spots. Retina. 1985. 5:206–214.
7. Chui TY, Thibos LN, Bradley A, Burns SA. The mechanisms of vision loss associated with a cotton wool spot. Vision Res. 2009. 49:2826–2834.
8. Ashton N. Pathological and ultrastructural aspects of the cotton-wool spots. Proc R Soc Med. 1969. 62:1271–1276.
9. Kozak I, Bartsch DU, Cheng L, Freeman WR. Hyperreflective sign in resolved cotton wool spots using high-resolution optical coherence tomography and optical coherence tomography ophthalmoscopy. Ophthalmology. 2007. 114:537–543.
10. Alencar LM, Medeiros FA, Weinreb R. Progressive localized retinal nerve fiber layer loss following a retinal cotton wool spot. Semin Ophthalmol. 2007. 22:103–104.
11. Gomez ML, Mojana F, Bartsch DU, Freeman WR. Imaging of long-term retinal damage after resolved cotton wool spots. Ophthalmology. 2009. 116:2407–2414.
12. Koh JW, Park KH, Kim MS, Kim JM. Localized retinal nerve fiber layer defects associated with cotton wool spots. Jpn J Ophthalmol. 2010. 54:296–299.
 XML Download
XML Download