

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To report a case of IgG4-related sclerosing dacryoadenitis masquerading for a long period as a.
Case summary
A 59-year-old man with visual acuity loss and proptosis in the left eye was referred to our hospital. Ten years prior, the patient was diagnosed with lymphoma and underwent chemotherapy at another hospital. However, the patient spontaneously stopped treatment and took steroids for the relief of periorbital swelling. Magnetic resonance imaging revealed diffuse infiltrative lesions involving both optic nerves and extraocular muscles. Incisional biopsies of the lacrimal gland's posterior side and the lateral rectus muscle's lateral side were performed. Staining for IgG4 via immunochemistry showed infiltration of IgG4-positive lymphoplasmacytic cells. Under the diagnosis of IgG4-related sclerosing disease, the patient underwent high-dose steroid pulse therapy.
Figures and Tables
Figure 1
Humphrey visual field test reveals marked visual field defects in the left eye (A), and inferior altitudinal visual field defects in the right eye (B).

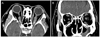
Figure 2
Orbit MRI reveals diffuse well enhancing infiltrative lesions involving both optic nerves, extraocular muscles, and cavernous sinus (A). Diffuse heterogeneous lesions involving the right maxillary sinus suggests sinusitis (B).

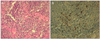
Figure 3
(A) Biopsied specimen shows interstitial fibrosis and lymphoplasmacytic infiltrations with lymphoid follicles (H&E, ×400). (B) Immunochemistry staining for IgG4 expression: IgG4-positive plasma cells have infiltrated the lesion (Anti-IgG4 Ab, ×400).

References
1. Kamisawa T, Funata N, Hayashi Y, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003. 38:982–984.
2. Yamamoto M, Takahashi H, Ohara M, et al. A new conceptualization for Mikulicz's disease as an IgG4-related plasmacytic disease. Mod Rheumatol. 2006. 16:335–340.
3. Sato Y, Ohshima K, Ichimura K, et al. Ocular adnexal IgG4-related disease has uniform clinicopathology. Pathol Int. 2008. 58:465–470.
4. Yamamoto M, Takahashi H, Sugai S, Imai K. Clinical and pathological characteristics of Mikulicz's disease (IgG4-related plasmacytic exocrinopathy). Autoimmun Rev. 2005. 4:195–200.
5. Kim K, Lee MJ, Kim NJ, et al. Three cases of Hyper-IgG4 syndrome involving ocular adnexa. J Korean Ophthalmol Soc. 2010. 51:1133–1138.
6. Okazaki K, Uchida K, Koyabu M, et al. Recent advances in the concept and diagnosis of autoimmune pancreatitis and IgG4-related disease. J Gastroenterol. 2011. 46:277–288.
7. Morgan WS, Castleman B. A clinicopathologic study of Mikulicz's disease. Am J Pathol. 1953. 29:471–503.
8. Tsubota K, Fujita H, Tsuzaka K, Takeuchi T. Mikulicz's disease and Sjögren's syndrome. Invest Ophthalmol Vis Sci. 2000. 41:1666–1673.
9. Hamano H, Kawa S, Ochi Y, et al. Hydronephrosis associated with retroperitoneal fibrosis and sclerosing pancreatitis. Lancet. 2002. 359:1403–1404.
10. Kitagawa S, Zen Y, Harada K, et al. Abundant IgG4-positive plasma cell infiltration characterizes chronic sclerosing sialadenitis (Küttner's tumor). Am J Surg Pathol. 2005. 29:783–791.
11. Naitoh I, Nakazawa T, Ohara H, et al. Endoscopic transpapillary intraductal ultrasonography and biopsy in the diagnosis of IgG4-related sclerosing cholangitis. J Gastroenterol. 2009. 44:1147–1155.
12. Hamano H, Kawa S, Ochi Y, et al. Hydronephrosis associated with retroperitoneal fibrosis and sclerosing pancreatitis. Lancet. 2002. 359:1403–1404.
13. Cheuk W, Chan JK. IgG4-related sclerosing disease: a critical appraisal of an evolving clinicopathologic entity. Adv Anat Pathol. 2010. 17:303–332.
14. Matsuo T, Ichimura K, Sato Y, et al. Immunoglobulin G4 (IgG4)-positive or -negative ocular adnexal benign lymphoid lesions in relation to systemic involvement. J Clin Exp Hematop. 2010. 50:129–142.
15. Thieblemont C, Bastion Y, Berger F, et al. Mucosa-associated lymphoid tissue gastrointestinal and nongastrointestinal lymphoma behavior: analysis of 108 patients. J Clin Oncol. 1997. 15:1624–1630.
16. Go H, Kim JE, Kim YA, et al. Ocular adnexal IgG4-related disease: comparative analysis with mucosa-associated lymphoid tissue lymphoma and other chronic inflammatory conditions. Histopathology. 2012. 60:296–312.
17. Kubota T, Moritani S, Yoshino T, et al. Ocular adnexal marginal zone B cell lymphoma infiltrated by IgG4-positive plasma cells. J Clin Pathol. 2010. 63:1059–1065.
18. Kubota T, Moritani S, Katayama M, Terasaki H. Ocular adnexal IgG4-related lymphoplasmacytic infiltrative disorder. Arch Ophthalmol. 2010. 128:577–584.
19. Kojima M, Sipos B, Klapper W, et al. Autoimmune pancreatitis: frequency, IgG4 expression, and clonality of T and B cells. Am J Surg Pathol. 2007. 31:521–528.
20. Takahira M, Kawano M, Zen Y, et al. IgG4-related chronic sclerosing dacryoadenitis. Arch Ophthalmol. 2007. 125:1575–1578.
21. Cheuk W, Yuen HK, Chan AC, et al. Ocular adnexal lymphoma associated with IgG4-+ chronic sclerosing dacryoadenitis: a previously undescribed complication of IgG4-related sclerosing disease. Am J Surg Pathol. 2008. 32:1159–1167.
22. Cheuk W, Yuen HK, Chan JK. Chronic sclerosing dacryoadenitis: part of the spectrum of IgG4-related Sclerosing disease? Am J Surg Pathol. 2007. 31:643–645.
23. Yamamoto M, Takahashi H, Ohara M, et al. A new conceptualization for Mikulicz's disease as an IgG4-related plasmacytic disease. Mod Rheumatol. 2006. 16:335–340.
 XML Download
XML Download