

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the long-term change of postoperative refraction after cataract surgery in patients with a history of LASIK.
Methods
A retrospective chart review was performed on 40 eyes of 28 patients who had undergone cataract surgery with a history of LASIK, and 40 eyes of 31 patients who had undergone cataract surgery without LASIK. We evaluated preoperative target refraction, and postoperative refraction during the 2-year follow-up period.
Results
In the group with a history of LASIK, the target refraction was -1.00 ± 0.98 D, the 2-month postoperative spherical equivalent was -0.53 ± 1.92 D, and the 2-year postoperative spherical equivalent was -1.03 ± 1.84 D. In the group with cataract surgery only, the target refraction was -1.44 ± 1.06 D, the 2-month postoperative spherical equivalent was -1.07 ± 1.27 D, and the 2-year postoperative spherical equivalent was -0.97 ± 1.28 D. The difference in mean spherical equivalent at 2 months postoperatively and at 2 years postoperatively between the 2 groups was statistically significant (p = 0.037). The difference in mean spherical equivalent preoperatively and 2 years postoperatively between the 2 groups was statistically significant (p = 0.002). In the group with cataract surgery only, the postoperative refraction shifted to hyperopic refractive power, and was statistically significant. In the group with a history of LASIK, there were no statistically significant differences between preoperative and postoperative refraction. There were no statistically significant differences according to the cataract type in the group with a history of LASIK. The greater the myopic preoperative spherical equivalent was, the shorter the duration between LASIK and cataract surgery, which was significant in the group with a history of LASIK.
Figures and Tables
Figure 1
Changes in mean spherical equivalent preoperatively and at 2 months and 2 years postoperatively in the group of cataract surgery after LASIK and the group of cataract surgery alone. *p < 0.05, paired t-test.

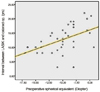
Figure 2
Scatter grams of preoperative spherical equivalent and time interval between cataract surgery and LASIK shows positive linear regression (Pearson correlation analysis, r2 = 0.478, p = 0.002).



References
1. Seitz B, Langenbucher A, Nguyen NX, et al. Underestimation of intraocular lens power for cataract surgery after myopic photorefractive keratectomy. Ophthalmology. 1999. 106:693–702.
2. Masket S, Masket SE. Simple regression formula for intraocular lens power adjustment in eyes requiring cataract surgery after excimer laser photoablation. J Cataract Refract Surg. 2006. 32:430–434.
3. Koch DD. New options for IOL calculations after refractive surgery. J Cataract Refract Surg. 2006. 32:371–372.
4. Langenbucher A, Haigis W, Seitz B. Difficult lens power calculations. Curr Opin Ophthalmol. 2004. 15:1–9.
5. Hamilton DR, Hardten DR. Cataract surgery in patients with prior refractive surgery. Curr Opin Ophthalmol. 2003. 14:44–53.
6. Helmy SA, Salah A, Badawy TT, Sidky AN. Photorefractive keratectomy and laser in situ keratomileusis for myopia between 6.00 and 10.00 diopters. J Refract Surg. 1996. 12:417–421.
7. Brint SF, Ostrick DM, Fisher C, et al. Six-month results of the multicenter phase I study of excimer laser myopic keratomileusis. J Cataract Refract Surg. 1994. 20:610–615.
8. Price FW Jr, Whitson WE, Gonzales JS, et al. Automated lamellar keratomileusis in situ for myopia. J Refract Surg. 1996. 12:29–35.
9. Chayet AS, Assil KK, Montes M, et al. Regression and its mechanisms after laser in situ keratomileusis in moderate and high myopia. Ophthalmology. 1998. 105:1194–1199.
10. McCarthy M, Gavanski GM, Paton KE, Holland SP. Intraocular lens power calculations after myopic laser refractive surgery: a comparison of methods in 173 eyes. Ophthalmology. 2011. 118:940–944.
11. Tsang CS, Chong GS, Yiu EP, Ho CK. Intraocular lens power calculation formulas in Chinese eyes with high axial myopia. J Cataract Refract Surg. 2003. 29:1358–1364.
12. Zaldivar R, Shultz MC, Davidorf JM, Holladay JT. Intraocular lens power calculations in patients with extreme myopia. J Cataract Refract Surg. 2000. 26:668–674.
13. Salah T, Waring GO 3rd, el Maghraby A, et al. Excimer laser in situ keratomileusis under a corneal flap for myopia of 2 to 20 diopters. Am J Ophthalmol. 1996. 121:143–155.
14. Magallanes R, Shah S, Zadok D, et al. Stability after laser in situ keratomileusis in moderately and extremely myopic eyes. J Cataract Refract Surg. 2001. 27:1007–1012.
15. Praveen MR, Shah GD, Vasavada AR, et al. A study to explore the risk factors for the early onset of cataract in India. Eye (Lond). 2010. 24:686–694.
16. Jeon S, Kim HS. Clinical characteristics and outcomes of cataract surgery in highly myopic Koreans. Korean J Ophthalmol. 2011. 25:84–89.
 XML Download
XML Download