

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To assess the efficacy of levator recession under local anesthesia to treat upper eyelid retraction.
Methods
Records of 12 patients (12 lids) were reviewed retrospectively. Postoperative cosmetic results were assessed as good, fair, or poor based on the upper lid height and symmetry. Preoperative and postoperative marginal reflex distance (MRD1, mm), upper eyelid asymmetry, lid lag, lagophthalmos, and ocular exposure symptoms were compared. The reoperation rate was also evaluated.
Results
Causes accounting for upper lid retraction were Graves ophthalmopathy (9 lids, 75.0%), orbital pseudotumor (2 lids, 16.7%), and hypercorrection from previous ptosis operation (1 lid, 8.3%). At a mean ± standard deviation of 27.7 ± 24.0 months follow-up (range, 5-60 months), 11 patients (91.7%) showed significantly better cosmetic results. MRD1 decreased an average of 3.1 ± 1.3 mm from 6.3 ± 1.5 mm preoperatively to 3.2 ± 0.9 mm postoperatively (p < 0.001). Upper lid asymmetry, lagophthalmos, and lid lag were also reduced significantly (p < 0.001). Overcorrection occurred in 3 lids (25%) and required levator advancement. Eleven patients (91.7%) experienced complete resolution of dry eye symptoms following levator recession.
Figures and Tables
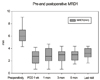 | Figure 1Preoperative and postoperative MRD1-time profiles. MRD1 levels were highest on the preoperative day, and decreased significantly after the levator recession.
|
 | Figure 2(A) Preoperative photograph of case 3, showing right upper eyelid retraction due to thyroid-associated ophthalmopathy. (B) Large amount of lid lag before levator recession. (C) Postoperative photograph showing dramatic improvement in eyelid level 1month after the operation. (D) Incision along the lid crease.
|
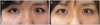 | Figure 3(A) Preoperative upper eyelid retraction in the left eye (case No. 4). (B) 4 months after the operation with good cosmetic result.
|

Table 2
Preoperative and postoperative data for patients undergoing levator recession for upper eyelid retraction

Values are presented as mean ± SD unless otherwise indicated.
*Calculation of p-values: paired samples t test and one-sample t test (after calculating delta values) were used for calculating preoperative and postoperative visual acuity, MRD1, and lagophthalmos differences; †Lid asymmetry was calculated as the absolute difference between both upper eyelids height (MRD1) preoperatively and postoperatively.
![]()
References
1. Clauser L, Galiè M, Sarti E, Dallera V. Rationale of treatment in Graves ophthalmopathy. Plast Reconstr Surg. 2001. 108:1880–1894.
2. Kagoshima T, Hori S, Inoue Y. Qualitative and quantitative analyses of Müller's muscle in dysthyroid ophthalmopathy. Jpn J Ophthalmol. 1987. 31:646–654.
3. Baldeschi L. Correction of lid retraction and exophthalmos. Dev Ophthalmol. 2008. 41:103–126.
4. Baylis HI, Cies WA, Kamin DF. Correction of upper eyelid retraction. Am J Ophthalmol. 1976. 82:790–794.
5. Putterman AM, Fett DR. Müller's muscle in the treatment of upper eyelid retraction: a 12-year study. Ophthalmic Surg. 1986. 17:361–367.
6. Grove AS Jr. Upper eyelid retraction and Graves' disease. Ophthalmology. 1981. 88:499–506.
7. Hedin A. Eyelid surgery in dysthyroid ophthalmopathy. Eye (Lond). 1988. 2(Pt 2):201–206.
8. Grove AS Jr. Eyelid retraction treated by levator marginal myotomy. Ophthalmology. 1980. 87:1013–1018.
9. Mourits MP, Koornneef L. Lid lengthening by sclera interposition for eyelid retraction in Graves' ophthalmopathy. Br J Ophthalmol. 1991. 75:344–347.
10. Elner VM, Hassan AS, Frueh BR. Graded full-thickness anterior blepharotomy for upper eyelid retraction. Arch Ophthalmol. 2004. 122:55–60.
11. Thaller VT, Kaden K, Lane CM, Collin JR. Thyroid lid surgery. Eye (Lond). 1987. 1(Pt 5):609–614.
12. McNab AA, Galbraith JE, Friebel J, Caesar R. Pre-Whitnall levator recession with hang-back sutures in Graves orbitopathy. Ophthal Plast Reconstr Surg. 2004. 20:301–307.
13. Hintschich C, Haritoglou C. Full thickness eyelid transsection (blepharotomy) for upper eyelid lengthening in lid retraction associated with Graves' disease. Br J Ophthalmol. 2005. 89:413–416.
14. Lee SH, Lew H, Yun YS. The result of botulinum toxin a injection in the upper eyelid retraction of thyroid-associated ophthalmopathy patients. J Korean Ophthalmol Soc. 2006. 47:1197–1203.
15. Lee JY. A statistical study on the corneal diameters in Korean. J Korean Ophthalmol Soc. 1983. 1:53–58.
16. Linberg JV, Vasquez RJ, Chao GM. Aponeurotic ptosis repair under local anesthesia. Prediction of results from operative lid height. Ophthalmology. 1988. 95:1046–1052.
17. Lee MJ, Oh JY, Choung HK, et al. Frontalis sling operation using silicone rod compared with preserved fascia lata for congenital ptosis a three-year follow-up study. Ophthalmology. 2009. 116:123–129.
18. Small RG. Surgery for upper eyelid retraction, three techniques. Trans Am Ophthalmol Soc. 1995. 93:353–365.
19. Ceisler EJ, Bilyk JR, Rubin PA, et al. Results of Müllerotomy and levator aponeurosis transposition for the correction of upper eyelid retraction in Graves disease. Ophthalmology. 1995. 102:483–492.
20. Tucker SM, Collin R. Repair of upper eyelid retraction: a comparison between adjustable and non-adjustable sutures. Br J Ophthalmol. 1995. 79:658–660.
 XML Download
XML Download