

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To report a case of neovascular glaucoma (NVG) with ocular ischemia in superior vena cava syndrome (SVCS).
Case summary
A 57-year old male who had been treated for small cell lung cancer (SCLC) visited our hospital because of SVCS-like symptoms and decreased visual acuity in the right eye. On the initial examination, best corrected visual acuity was 0.5, intraocular pressure (IOP) was 38 mm Hg and relative afferent papillary defect was positive in the right eye. Slit lamp examination showed mild dilatation and tortuosity of the episcleral vessels and ruobeosis iridis. Gonioscopic examination showed neovascularization of the opened angle. Fluorescein angiography showed delayed choroidal filling and nevascularization of the disc. The patient was diagnosed with NVG with ocular ischemia in SVCS and was treated with chemotherapy and steroid therapy. In addition, intravitreal bevacizumab and IOP lowering eyedrops were administered to the right eye. During follow-up, neovascularizations disappeared and IOP was well controlled.
Figures and Tables
Figure 1
(A) Brain magnetic resonance imaging shows multiple metastasis of the small cell lung cancer. (B) The coronal view of chest computed tomography shows compression of the superior vena cava (lower arrow) and the right internal jugular vein (upper arrow) by lymphadenopathy and distention of the right internal jugular vein (upper arrow). The axial views of chest computed tomography show that (C) decreased diameter of the superior vena cava surrounded by lymphadenopathy and (D) diameter of the right common carotid artery (left arrow) near by lymphadenopathy was smaller than which of the left common carotid artery (right arrow).

Figure 2
Slit lamp and gonioscopic exam of right eye (A, B) and left eye (C, D). (A) Mild dilatation and tortuosity of the episcleral vessels of right eye (arrows). (B) Neovascularization of the angle (rectangle). (C) Mild dilatation and tortuosity of the episcleral vessels of left eye (arrows). (D) No specific finding of the angle.
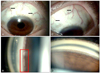
Figure 3
Fundus photograph and fluorescein angiograph of right eye (A, B, C) and left eye (D, E, F). (A) Dot shaped hemorrhagies and neovascularization of the disc (NVD). (B) Fillings of the choroid and the retinal artery were started at 32 seconds after injection. (C) Filling of the temporal retinal vein was completed at 1 minute 11 seconds. Multiple microaneurysms and leaking around the disc. (D) Dot shaped hemorrhagies. (E) Venous phase shows multiple microaneurysms. (F) Late phase shows only multiple microaneurysms too.

References
1. Gauden SJ. Superior vena cava syndrome induced by bronchogenic carcinoma: is this an oncological emergency? Australas Radiol. 1993. 37:363–366.
2. Bell DR, Woods RL, Levi JA. Superior vena caval obstruction: a 10-year experience. Med J Aust. 1986. 145:566–568.
3. Brubaker RF. Determination of episcleral venous pressure in the eye. A comparison of three methods. Arch Ophthalmol. 1967. 77:110–114.
4. Kollarits CR, Gaasterland D, Di Chiro G, Christiansen J, Yee RD. Management of a patient with orbital varices, visual loss, and ipsilateral glaucoma. Ophthalmic Surg. 1977. 8:54–62.
5. Greenfield DS. Glaucoma associated with elevated episcleral venous pressure. J Glaucoma. 2000. 9:190–194.
6. Kearns TP, Hollenhorst RW. Venous-stasis retinopathy of occlusive disease of the carotid artery. Proc Staff Meet Mayo Clin. 1963. 38:304–312.
7. Brown GC, Magargal LE. The ocular ischemic syndrome. Clinical, fluorescein angiographic and carotid angiographic features. Int Ophthalmol. 1988. 11:239–251.
8. Mun SJ, Lee KH, Lee DU, Cho NC. Clinical features of ophthalmic artery hypoperfusion. J Korean Ophthalmol Soc. 2007. 48:297–302.
9. Sivalingam A, Brown GC, Megargal LE. The ocular ischemic syndrome. III. Visual prognosis and the effect of treatment. Int Ophthalmol. 1991. 15:15–20.
10. Amselem L, Montero J, Diaz-Llopis M, et al. Intravitreal bevacizumab (Avastin) injection in ocular ischemic syndrome. Am J Ophthalmol. 2007. 144:122–124.
11. Nakase H, Heimann A, Kempski O. Alterations of regional cerebral blood flow and oxygen saturation in a rat sinus-vein thrombosis model. Stroke. 1996. 27:720–727.
12. Nakase H, Nagata K, Otsuka H, et al. Local cerebral blood flow autoregulation following "asymptomatic" cerebral venous occlusion in the rat. J Neurosurg. 1998. 89:118–124.
13. Nakase H, Kempski OS, Heimann A, et al. Microcirculation after cerebral venous occlusions as assessed by laser Doppler scanning. J Neurosurg. 1997. 87:307–314.
14. Rodriguez RA, Cornel G, Austin EH 3rd, et al. Brain function monitoring during bidirectional Glenn procedures. J Thorac Cardiovasc Surg. 2000. 119:617–619.
15. Masuda H, Ogata T, Kikuchi K. Physiological changes during temporary occlusion of the superior vena cava in cynomolgus monkeys. Ann Thorac Surg. 1989. 47:890–896.
16. Urayama H, Kawase Y, Ohtake H, et al. Physiological changes during acute obstruction of the superior vena cava, azygos, and internal thoracic veins in dogs. J Cardiovasc Surg (Torino). 1997. 38:87–92.
17. Hsu HY, Chao AC, Chen YY, et al. Reflux of jugular and retrobulbar venous flow in transient monocular blindness. Ann Neurol. 2008. 63:247–253.
 XML Download
XML Download