

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the amount of excyclotorsion according to degree of inferior oblique overaction (IOOA) in patients with primary IOOA.
Methods
Fifty-nine primary IOOA patients who underwent inferior oblique muscle surgery were evaluated. Visual acuity, ocular movement test, prism cover test, Bielschowsky head tilt test, fundus photograph and photographic examination for excyclotorsion were performed. The correlation analysis was performed for the excyclotorsion according to the amount of IOOA (Control group; IOOA < 1, Group 1; 1 ≤ IOOA < 2, Group 2; 2 ≤ IOOA < 3, Group 3; 3 ≤ IOOA < 4, Group 4; IOOA = 4).
Results
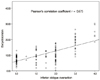
Excyclotorsion was 7.37 ± 2.36° in the Control group, 9.29 ± 3.79° in Group 1, 10.04 ± 4.39° in Group 2, 17.98 ± 4.62° in Group 3, and 24.70 ± 4.61° in Group 4. The amount of IOOA and excyclotorsion showed a positive correlation (Pearson's correlation coefficient r = 0.675). Asymmetric IOOA was observed in 35 patients (59.3%) and symmetric IOOA was observed in 24 patients (40.7%). Asymmetric IOOA combined with hypertropia was presented in 9 patients (37.5%) and symmetric IOOA combined with hypertropia was presented in 3 patients (8.6%). Therefore, patients with asymmetric IOOA have a higher incidence of vertical diplopia. The amounts of IOOA and excyclotorsion were greater in primary IOOA with esotropia than in subjects with exotropia (p = 0.001).
Figures and Tables





References
1. Von Noorden GK, Campos EC. Binocular Vision and Ocular Motility : Theory and Management of Strabismus. 2002. 6th ed. St Louis: Mo Mosby;55–56.
2. Guyton DL, Weingarten PE. Sensory torsion as the cause of primary oblique muscle overaction/underaction and A-and V-pattern strabismus. Binocul Vis Eye Muscle Surg Q. 1994. 9:209–236.
3. Knapp P. Vertically incomitant horizontal strabismus: the so-called "A" and "V" syndromes. Trans Am Ophthalmol Soc. 1959. 57:666–699.
4. Eustis HS, Nussdorf JD. Inferior oblique overaction in infantile esotropia: fundus extorsion as a predictive sign. J Pediatr Ophthalmol Strabismus. 1996. 33:85–88.
5. Bixenman WW, von Noorden GK. Apparent foveal displacement in normal subjects and in cyclotropia. Ophthalmology. 1982. 89:58–62.
6. Morton GV, Lucchese N, Kushner BJ. The role of funduscopy and fundus photography in strabismus diagnosis. Ophthalmology. 1983. 90:1186–1191.
7. Duane A. Binocular movements. Arch Ophthalmol. 1933. 9:579–607.
8. Scobee RG. The oculorotary muscles. Mosby. 1958. 2:264–268.
9. Parks MM. Inferior oblique weakening procedures. Int Ophthalmol Clin. 1985. 25:107–117.
10. Lee DH, Lee SJ, Park SH. Ocular torsion in normal Korean population. J Korean Ophthalmol Soc. 2004. 45:797–802.
11. Lee HJ, Lim KH. The range of ocular torsion in mass screening. J Korean Ophthalmol Soc. 2005. 46:1684–1689.
12. Song MH, Lee SY, Lee YC. The relationship of hypertropia, inferior oblique overaction and extorsion in congenital superior oblique palsy. J Korean Ophthalmol Soc. 2007. 48:1394–1398.
13. Kim EH, Lee SJ, Choi HY. Ocular torsion according to fixation in fundus photograph. J Korean Ophthalmol Soc. 2006. 47:449–454.
14. Kushner BJ, Kraft SE, Vrabec M. Ocular torsional movements in humans with normal and abnormal ocular motility--Part I: Objective measurements. J Pediatr Ophthalmol Strabismus. 1984. 21:172–177.
15. Chang BL. Superior oblique palsy. J Korean Ophthalmol Soc. 1991. 32:300–306.
16. Guyton DL. Clinical assessment of ocular torsion. Am Orthopt J. 1983. 33:7–15.
17. Wilson ME, Parks MM. Primary inferior oblique overaction in congenital esotropia, accommodative esotropia, and intermittent exotropia. Ophthalmology. 1989. 96:950–955.
18. Kim JW, Kim MM. The effect of inferior oblique weakening procedures in the congenital superior oblique palsies. J Korean Ophthalmol Soc. 2004. 45:1893–1898.
19. Chang BL, Chang MH, Yang SW. Inferior oblique overaction. J Korean Ophthalmol Soc. 1988. 29:1065–1069.
20. Min BM, Park JH. Comparison between myectomy and anterior transposition on inferior oblique overaction. J Korean Ophthalmol Soc. 1992. 33:977–982.
21. Rah SH, Jun HS, Kim SH. An epidemiologic survey of strabismus among school-children in Korea. J Korean Ophthalmol Soc. 1997. 38:2195–2199.
22. Steffen H, Straumann DS, Walker MF, et al. Torsion in patients with superior oblique palsies: dynamic torsion during saccades and changes in Listing's plane. Graefes Arch Clin Exp Ophthalmol. 2008. 246:771–778.
 XML Download
XML Download