

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To report a case of keratitis caused by Acinetobacter baumannii and Candida parapsilosis in a patient using 0.5% levofloxacin and 0.1% fluorometholone for an extended period of time.
Case summary
A 55-year-old male patient in the neurosurgery department with conjunctival injection and discharge in his left eye was consulted for ophthalmic evaluation and treatment. He was hospitalized in the state of akinetic mutism and given 0.5% levofloxacin and 0.1% fluorometholone for 2 years. On slit-lamp examination, a 3.5 × 4.5-mm dense stromal infiltrate with an overlying epithelial defect was observed. Corneal scraping culture revealed multidrug-resistant A. baumannii and C. parapsilosis. According to the susceptibility result, the patient was treated with topical 10% piperacillin/tazobactam and 0.125% amphotericin B hourly. The corneal ulcer healed gradually with corneal opacity remaining after 8 weeks of treatment.
Figures and Tables
Figure 1
Anterior segment photographs on the first ophthalmic examination showing severe conjunctival injection, corneal stromal infiltration, corneal scar and neovascularization (arrows).

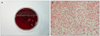
Figure 2
Characteristics of A. baumannii. Initial photograph shows multiple colonies on MacConkey agar, each colony shows non-pigmented, dome-shaped cluster (A), Gram-stain showed gram-negative coccobacilli (B).


References
1. Peleg AY, Seifert H, Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clin Microbiol Rev. 2008. 21:538–582.
2. Peleg AY, Paterson DL. Multidrug-resistant Acinetobacter: a threat to the antibiotic era. Intern Med J. 2006. 36:479–482.
3. Kim ST, Lee YC, Heo J, Koh JW. A case of Acinetobacter baumannii keratitis after contact lens wearing. J Korean Ophthalmol Soc. 2008. 49:1696–1700.
4. Kim HD, Kim SY, Jung MS. A case of Candida parapsilosis keratitis with atypical presentation. J Korean Ophthalmol Soc. 2010. 51:136–140.
5. Bouvet PJM, Grimont PAD. Taxonomy of the genus Acinetobacter with the recognition of Acinetobacter baumannii sp. nov., Acinetobacter haemolyticus sp. nov., Acinetobacter johnsonii sp. nov., and Acinetobacter junii sp. nov., and emended descriptions of Acinetobacter calcoaceticus and Acinetobacter lwoffii. Int J Syst Bacteriol. 1986. 36:228–240.
6. Gómez J, Simarro E, Baños V, et al. Six-year prospective study of risk and prognostic factors in patients with nosocomial sepsis caused by Acinetobacter baumannii. Eur J Clin Microbiol Infect Dis. 1999. 18:358–361.
7. Marcovich A, Levartovsky S. Acinetobacter exposure keratitis. Br J Ophthalmol. 1994. 78:489–490.
8. Herbst RW. Herellea corenal ulcer associated with the use of soft contact lenses. Br J Ophthalmol. 1972. 56:848–850.
9. Kent HD, Cohen EJ, Laibson PR, Arentsen JJ. Microbial keratitis and corneal ulceration associated with therapeutic soft contact lenses. CLAO J. 1990. 16:49–52.
10. Zabel RW, Winegarden T, Holland EJ, Doughman DJ. Acinetobacter corneal ulcer after penetrating keratoplasty. Am J Ophthalmol. 1989. 107:677–678.
11. Presley GD, Hale LM. Corneal ulcer due to Bacterium anitratum. Am J Ophthalmol. 1968. 65:571–572.
12. Sung H, Choi SJ, Yoo S, Kim MN. [In vitro antimicrobial synergy against imipenem-resistant Acinetobacter baumannii]. Korean J Lab Med. 2007. 27:111–117.
13. Kim JH, Kim HB, Kim JC, et al. Corea. 1999. 2nd ed. Seoul: Ilchokak;109–126.
14. Hahn YH, Lee DJ, Kim MS, et al. Epidemiology of fungal keratitis in Korea: a multi-center study. J Korean Ophthalmol Soc. 2000. 41:1499–1508.
15. Sun RL, Jones DB, Wilhelmus KR. Clinical characteristics and outcome of Candida keratitis. Am J Ophthalmol. 2007. 143:1043–1045.
16. Bourcier T, Touzeau O, Thomas F, et al. Candida parapsilosis keratitis. Cornea. 2003. 22:51–55.
17. Chew FL, Soong TK, Shin HC, et al. Topical piperacillin/tazobactam for recalcitrant pseudomonas aeruginosa keratitis. J Ocul Pharmacol Ther. 2010. 26:219–222.
18. Srinivasan M. Fungal keratitis. Curr Opin Ophthalmol. 2004. 15:321–327.
 XML Download
XML Download