

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background/Aims
Methods
Results
Conclusions
Figures and Tables
 | Fig. 1Flow of the study. Of the 7,178 included subjects, 274 (3.8%) showed an equivocal H. pylori serology test finding. Of the 98 subjects followed-up with an equivocal test finding, 58 (59.2%) showed seroconversion. H. pylori, Helicobacter pylori; IgG, immunoglobulin G.
|
Table 1
Baseline Characteristics of the Followed-up Subjects with an Equivocal H. pylori Test Finding

Values are presented as mean±standard deviation or n (%) unless otherwise indicated.
H. pylori, Helicobacter pylori.
ap-values show the differences between 58 subjects with seroconversion and 40 subjects without seroconversion. Continuous variables are shown as mean value±standard deviation using the Student's t-test. Categorical variables are shown in frequency (%) using the Chi-square test or Fisher's exact test; b≥15 drinks/week for men, ≥8 drinks/week for women.
![]()
Table 2
Initial and Follow-up Test Findings of Subjects according to the Follow-up Serum Anti-H. pylori IgG Test Finding

Variables are shown as mean value±standard deviation using the Student's t-test.
H. pylori, Helicobacter pylori; IgG, immunoglobulin G; PG, pepsinogen.
ap-values indicate differences between the subjects with seroconversion and without seroconversion; bp-values indicate differences between the initial and follow-up test findings using the signed-rank test.
![]()
Table 3
Differences between Subjects with a Negative Test Finding and Those with an Equivocal Test Finding

Values are presented as mean±standard deviation or n (%) unless otherwise indicated. Continuous variables are shown as mean value±standard deviation using the Student's t-test. Categorical variables are shown in frequency (%) using the Chi-square test or Fisher's exact test.
H. pylori, Helicobacter pylori; PG, pepsinogen.
![]()
Table 4
Findings of Subjects with a History of H. pylori Eradication
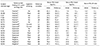
Upward arrow (↑) indicates that there was a synchronous increase in serum PG I and PG II levels during the follow-up period, whereas downward (↓) indicates vice versa.
H. pylori, Helicobacter pylori; M, male; F, female; PG, pepsinogen.
aSix subjects showed seroconversion at the follow-up test, although the initial serum PG I and PG II levels were low. Most showed decreasing trends of serum PG levels at the follow-up tests, suggesting that seroconversion is related to slow IgG clearance at posteradication period; bThree subjects showed increasing trends of serum PG levels at the follow-up tests, suggesting that there is a reinfection or recrudescence in these subjects; cTwo subjects showed seroreversion despite their high initial serum PG levels. Decreasing trends of serum PG I and PG II levels in these subjects suggest that initial equivocal test findings in these subjects were due to the delayed seroreversion after eradication.
![]()
 XML Download
XML Download