

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Esophageal duplication cyst is a rare congenital gastrointestinal malformation. It is the second most common duplication cyst following small bowel duplication cyst in the gastrointestinal tract. Patients with an esophageal duplication cyst are generally asymptomatic; however, some patients may present the following symptoms: dysphagia, chest pain, stridor, unproductive cough, and epigastric discomfort by compression of the surrounding structures. Surgical removal is the treatment of choice in symptomatic cases and can be considered in asymptomatic cases if they are at risk for developing complications, such as ulceration or perforation. Herein, we report a case of hemorrhage of an esophageal duplication cyst, which was improved by endoscopic drainage.
Figures and Tables
Fig. 1
Chest computed tomography (CT). (A) Initial chest CT. A large cystic mass with inner high density suggesting hematoma is observed at the posterior mediastinum, and this mass compresses the lower esophagus. (B) Follow-up chest CT after operation. Previous cystic mass is still observed, but with slightly reduced size.
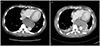
Fig. 2
Emergent intra-operative thoracoscopy. (A) Mediastinum is clear, and the external surface of the esophagus is intact. However, the esophagus is markedly swollen. (B) After incision of the esophagus, a large amount of hematoma is found in the esophageal wall, but the esophageal muscular, submucosal, and mucosal layers are intact.

Fig. 3
Endoscopic drainage. (A) A subepithelial lesion with positive cushion sign (arrow) is observed at the lower esophagus. (B) On endoscopic ultrasonography, the lesion is a 7.6 cm-sized cystic lesion located at the muscular layer of the esophagus, and a large amount of hyperechoic floating materials are observed inside the cystic lesion. (C) Mucosal and submucosal incision is performed using a dual knife. (D) A large amount of hematoma and pus are found inside the lesion. These hematoma and pus are removed via repetitive endoscopic aspiration and saline washing.
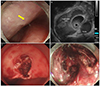
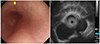
Fig. 4
Follow-up endoscopy and endoscopic ultrasonography (EUS) at 4 months after endoscopic drainage. (A) On endoscopy, the previous subepithelial lesion is markedly decreased, and the incision site is completely healed (arrow). (B) On EUS, the cystic lesion is still observed at the muscular layer of the esophagus, but its size decreases to 3.7 cm and the previous hyperchoic floating materials are not seen any more.
References
1. Liu R, Adler DG. Duplication cysts: diagnosis, management, and the role of endoscopic ultrasound. Endosc Ultrasound. 2014; 3:152–160.
2. Whitaker JA, Deffenbaugh LD, Cooke AR. Esophageal duplication cyst. Case report. Am J Gastroenterol. 1980; 73:329–332.
3. Salo JA, Ala-Kulju KV. Congenital esophageal cysts in adults. Ann Thorac Surg. 1987; 44:135–138.
4. Nobuhara KK, Gorski YC, La Quaglia MP, Shamberger RC. Bronchogenic cysts and esophageal duplications: common origins and treatment. J Pediatr Surg. 1997; 32:1408–1413.
5. Bhatia V, Tajika M, Rastogi A. Upper gastrointestinal submucosal lesions--clinical and endosonographic evaluation and management. Trop Gastroenterol. 2010; 31:5–29.
6. Ildstad ST, Tollerud DJ, Weiss RG, Ryan DP, McGowan MA, Martin LW. Duplications of the alimentary tract. Clinical characteristics, preferred treatment, and associated malformations. Ann Surg. 1988; 208:184–189.
7. Bowton DL, Katz PO. Esophageal cyst as a cause of chronic cough. Chest. 1984; 86:150–152.
8. Cioffi U, Bonavina L, De Simone M, et al. Presentation and surgical management of bronchogenic and esophageal duplication cysts in adults. Chest. 1998; 113:1492–1496.
9. Geller A, Wang KK, DiMagno EP. Diagnosis of foregut duplication cysts by endoscopic ultrasonography. Gastroenterology. 1995; 109:838–842.
10. Diehl DL, Cheruvattath R, Facktor MA, Go BD. Infection after endoscopic ultrasound-guided aspiration of mediastinal cysts. Interact Cardiovasc Thorac Surg. 2010; 10:338–340.
11. Wildi SM, Hoda RS, Fickling W, et al. Diagnosis of benign cysts of the mediastinum: the role and risks of EUS and FNA. Gastrointest Endosc. 2003; 58:362–368.
12. Ivekovic H, Jouret-Mourin A, Deprez PH. Endoscopic fenestration of esophageal duplication cysts. Endoscopy. 2012; 44:Suppl 2 UCTN. E404–E405.
13. Mou Y, Wen D, Liu Q, et al. Endoscopic resection of an esophageal duplication cyst with spraying of anhydrous alcohol. Endoscopy. 2015; 47:Suppl 1 UCTN. E348–E349.
 XML Download
XML Download