

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Collision tumors of the colon are rare. A 54-year-old man was referred to our hospital for the evaluation of hematochezia. Colonoscopy demonstrated the presence of about 3 cm sized mass in the rectosigmoid junction. After surgical resection, the colonic lesion was histologically composed of two discrete lesions: adenocarcinoma in the superficial layer and poorly differentiated neuroendocrine carcinoma in the deeper layer. We report this case of colonic collision tumor (adenocarcinoma and neuroendocrine carcinoma) with a review of the literature.
Figures and Tables
 | Fig. 1Colonoscopic finding. It showed about 3 cm sized ulcerofungating mass in the rectosigmoid junction.
|
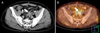
 | Fig. 2Abdominal CT finding. An about 3 cm sized intraluminal enhancing mass was seen on the rectosigmoid junction without streaky densities in surrounding pericolic fat tissue.
|
 | Fig. 3Laparoscopic finding. It showed serosal infiltration of the mass in the rectosigmoid junction (arrowheads).
|

References
1. Bernick PE, Klimstra DS, Shia J, et al. Neuroendocrine carcinomas of the colon and rectum. Dis Colon Rectum. 2004. 47:163–169.
2. Chang JH, Kim SW, Chung WC, et al. Clinical review of gastrointestinal carcinoid tumor and analysis of the factors predicting metastasis. Korean J Gastroenterol. 2007. 50:19–25.
3. Kang BS, Kim JW. Gastrointestinal carcinoid tumor: Clinical review of 36 cases. J Korean Surg Soc. 2009. 76:1–6.
4. Lee MH, Shin SJ, Jeon SJ, et al. Clinical characteristics of gastrointestinal carcinoid tumors. Korean J Gastrointest Endosc. 2010. 40:347–351.
5. Gould VE, Chejfec G. Neuroendocrine carcinomas of the colon. Ultrastructural and biochemical evidence of their secretory function. Am J Surg Pathol. 1978. 2:31–38.
6. Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas. 2010. 39:707–712.
7. Rindi G, Capella C, Solcia E. Introduction to a revised clinicopathological classification of neuroendocrine tumors of the gastroenteropancreatic tract. Q J Nucl Med. 2000. 44:13–21.
8. Yamashina M, Flinner RA. Concurrent occurrence of adenocarcinoma and carcinoid tumor in the stomach: a composite tumor or collision tumors? Am J Clin Pathol. 1985. 83:233–236.
9. Fukui H, Takada M, Chiba T, et al. Concurrent occurrence of gastric adenocarcinoma and duodenal neuroendocrine cell carcinoma: a composite tumour or collision tumours? Gut. 2001. 48:853–856.
10. Olinici CD, Domşa I, Crişan D. Collision adenocarcinoma-- carcinoid tumor of the colon. Case report and review of the literature. Rom J Morphol Embryol. 2007. 48:75–78.
11. Pecorella I, Memeo L, Ciardi A, Rotterdam H. An unusual case of colonic mixed adenoendocrine carcinoma: collision versus composite tumor. A case report and review of the literature. Ann Diagn Pathol. 2007. 11:285–290.
12. Lyda MH, Fenoglio-Preiser CM. Adenoma-carcinoid tumors of the colon. Arch Pathol Lab Med. 1998. 122:262–265.
13. Moyana TN, Qizilbash AH, Murphy F. Composite glandular-carcinoid tumors of the colon and rectum. Report of two cases. Am J Surg Pathol. 1988. 12:607–611.
14. Mills SE, Allen MS Jr, Cohen AR. Small-cell undifferentiated carcinoma of the colon. A clinicopathological study of five cases and their association with colonic adenomas. Am J Surg Pathol. 1983. 7:643–651.
15. Staren ED, Gould VE, Jansson DS, Hyser M, Gooch GT, Economou SG. Neuroendocrine differentiation in "poorly differentiated" colon carcinomas. Am Surg. 1990. 56:412–419.
16. Saclarides TJ, Szeluga D, Staren ED. Neuroendocrine cancers of the colon and rectum. Results of a ten-year experience. Dis Colon Rectum. 1994. 37:635–642.
17. Moertel CG, Kvols LK, O'Connell MJ, Rubin J. Treatment of neuroendocrine carcinomas with combined etoposide and cisplatin. Evidence of major therapeutic activity in the anaplastic variants of these neoplasms. Cancer. 1991. 68:227–232.
18. Okuyama T, Korenaga D, Tamura S, et al. The effectiveness of chemotherapy with cisplatin and 5-fluorouracil for recurrent small cell neuroendocrine carcinoma of the rectum: report of a case. Surg Today. 1999. 29:165–169.
 XML Download
XML Download