

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Squamous cell carcinoma of the esophagus is occasionally associated with malignancies of other organs and regions of the body, such as the head and neck, the upper respiratory tract and the rest of the digestive tract.1,2 In Japan, esophageal squamous cell carcinoma is frequently associated with adenocarcinoma of the stomach.3 Recently, the frequency of synchronous esophageal and gastric cancer was reported increasing, due to the development of more sophisticated invasive and non-invasive diagnostic tools and to an increase in the number of elderly patients.4 Although the optimal management of simultaneous gastric and esophageal cancer was not established yet, principle of treatment was radical resection of each cancer, such as total gastrectomy with esophagectomy.5,6 However, to date, cases of successfully treatment of synchronous esophageal and stomach cancer using chemotherapy have been rarely reported. We report here a case of a patient with synchronous esophageal and gastric cancer who achieved and sustained complete remission following combination chemotherapy with docetaxel and cis-diammineedichloro-platinum (CDDP).
CASE REPORT
A 82-year-old man was admitted to our hospital on September 23, 2008, he was complaining of anorexia and progressive weight loss of 7 kg in the past 6 months. On admission, he was 178 cm tall and weighed 60 kg, and no specific clinical findings were noted. He had arterial hypertension and healed pulmonary tuberculosis. His brother died due to advanced stomach cancer. He was a heavy alcohol consumer. Performance status on the Eastern Cooperative Oncology Group (ECOG) scale was rated 1.
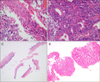
There were no abnormal findings in the laboratory data, including tumor markers. Chest X-ray showed increased opacity with decreased lung volume in the right upper lobe. Amorphous calcifications were present in the left apex and pleural thickening with calcification in the left lower lobe was seen. We performed pulmonary function test, and found a severe obstructive lung defect, FEV1/FVC 58%, FEV1 0.76 L and FEF 25-75% 0.35 L/sec. Endoscopy revealed an elevated lesion 30-35 cm from the incisor teeth, on the left-anterior wall of the lower esophagus (Fig. 1A). An 'unstained area' delineated the lesion and the surrounding flat lesion on endoscopy with iodine staining (Fig. 1B). The specimen taken from the tumor revealed moderately differentiated squamous cell carcinoma (Fig. 2A). Simultaneously, superficially flat and erythematous lesion was detected in the mid antrum lesser curvature of the stomach (Fig. 1C). Biopsy of the gastric lesion showed moderately differentiated adenocarinoma (Fig. 2B). The chest CT image showed diffuse wall thickening of the lower esophagus and enlargement of the paratracheal lymph node. The abdominal CT image suggested single lymph node enlargement in the left perigastric area (Fig. 3A). The PET-CT revealed increased flurodeoxyglucose (FDG) uptake in the lower esophagus, the mediastinal lymph node and the para-aortic lymph node. However, there was no FDG uptake in the stomach and no other distant organ metastasis (Fig. 3B). The preoperative radiologic staging was T2N1M0, stage IIB esophageal cancer and T1N1M0, stage IB gastric cancer; both cancers were diagnosed as surgically resectable. However, surgery was contraindicated because of severe lung dysfunction. Moreover, the patient refused both radiotherapy and endoscopic management due to high-cost. Therefore, the patient was given combined chemotherapy with docetaxel and cisplatin.
Chemotherapy was started on November 7, 2008. On day 1, docetaxel (65 mg/m2) was administrated by intravenous infusion for 60 minutes, followed by intravenous infusion of CDDP (60 mg/m2) for 15 minutes, with adequate hydration. The treatment was repeated every 3 weeks. He received three cycles of chemotherapy, without showing any severe toxic side effects. After three cycles of chemotherapy, the endoscopic examinaton showed complete disappearance of both the esophageal mass and the stomach cancer, and only a remnant scar (Fig. 4). There were no tumor cells on pathologic examination (Fig. 2C, D). The chest and abdominal CT scans also showed marked decrease of the lymph node metastasis. This combination chemotherapy was continued further, with close follow-up examinations, and the same treatment was repeated every 3-4 weeks. In total, the patient received ten cycles of chemotherapy, without severe adverse effects, until May 2009. The metastatic lymph nodes completely disappeared on the CT scan and FDG uptake was not detected on the PET-CT scan (Fig. 3C, D). The patient survived for 18 months after discontinuation of the chemotherapy, without any apparent recurrence.
Discussion
The patient showed complete remission of the synchronous esophagus and stomach cancers after combined chemotherapy with docetaxel plus CDDP. Furthermore, complete remission was confirmed on endoscopic biopsy. This case was a rare report of successful treatment in synchronous esophagus and stomach cancer, using combination chemotherapy instead of surgery.
In Japan, according to reports from the literature, the incidence of synchronous associated gastric cancer is reported to be up to 3.9-6.1% in esophageal cancer patients.5-7 However, it is not easy to explain the simultaneous occurrence of two malignancies in different but adjacent parts of the upper digestive tract, considering that the esophagus and the stomach have different histological structures and the epidemiology is different. Generally, the synchronous occurrence of cancers has been explained by the concept of field carcinogenesis. The esophageal and gastric cancers share some risk factors, including diet, low socioeconomic status, age, alcohol and tobacco use and nitrate exposure.4 Our patient was indeed a heavy alcohol consumer.
Although the optimal management of the simultaneous gastric and esophageal cancers has not been established yet, radical resection for both cancers, i.e., esophagectomy with total gastrectomy were usually recommended, especially in the advanced stage.5,6 However, esophagectomy and total gastrectomy are a huge burden with high risk, especially in old patients. To lighten the burden, new techniques for reducing the scale of the treatment have been developed. For the early gastric cancer of the upper third of the stomach, esophagectomy with esophago-gastric anastomosis after proximal gastrectomy with lymph node dissection was demonstrated useful.5 When the synchronous esophageal and gastric cancers are confined to the mucosa, without lymph node metastasis, either endoscopic mucosal resection (EMR) of both lesions or EMR of the gastric cancer followed by surgery on the esophageal cancer could be the adequate treatment.8,9
If either surgery or endoscopic treatment is impossible, like in the presented case, chemotherapy might be an alternative choice. In Japan, to date, we found only two case reports of synchronous cancers of the esophagus and the stomach successfully treated with combination chemotherapy. One case was treated using TS-1 plus cisplatin and the other case was treated using 5-fluorouracil plus consecutive low-dose cisplatin.10,11 We have chosen docetaxel plus cisplatin combination chemotherapy. Because, in previous studies, this combination chemotherapy has shown a very potent antitumor activity against both esophageal squamous cancer and gastric adenocarcinoma and was well tolerated with manageable toxicity. Docetaxel, a semisynthetic taxoid developed in the eighties, is derived from the needles of the European yew tree, Taxus baccata.12 It enhances the microtubule assembly and inhibits the depolymerisation of tubulin. Docetaxel has shown antitumor activity against various common cancers, including ovarian, breast, gastric, head and neck, and lung cancers.13 In vitro studies with docetaxel have shown a lack of cross resistance to cisplatin, etoposide and 5-fluorouracil.14 Myelosuppression is a dose-limiting toxicity of docetaxel, whereas myelotoxicity with cisplatin is mild. Like this, since the toxicity profiles of docetaxel and cisplatin showed little significant overlap, a combination of these agents seemed to constitute a logical step of investigation. A phase II study of docetaxel plus cisplatin as first-line therapy in patients with metastatic squamous esophageal cancer showed the response rate of 33.3%, the median progression free survival of 5.0 months and the median overall survival rate of 8.3 months.15 Another study showed a similarly good efficacy.16 In addition, in metastatic or locally advanced gastric adenocarcinoma, this combination chemotherapy showed very potent efficacy. Overall, the response rates were from 26% to 43.5%, the mean time to progression was from 5.0 to 7.0 months and the median overall survival rate was from 9.0 to 11.5 months.17-20 We used each agent at doses of docetaxel 65 mg/m2 and cisplatin 60 mg/m2, which was lower dose intensity than dose in current use, docetaxel 70-85 mg/m2, cisplatin 70-80 mg/m2.15-20 Because the patient was 82-year-old with severe lung dysfunction and older patients appear to be at special risk for severe and prolonged myelosuppression and mucositis, as well as increased risk of infection as a side effect of the chemotherapy, chemotherapy was started with 25% dose reduction and maintained without serious adverse effect.
In general, chemotherapy plays a major role in the palliative therapy and is still the primary mode of treatment for the recurrent metastatic esophageal or gastric cancer. Although both tumors were resectable, the presented case was a rare report of successful, non-surgical treatment, using chemotherapy in synchronous esophagus and stomach cancers. Surgery or endoscopic treatment of both the esophageal and gastric cancers is desirable, however, if they prove medically inoperable, chemotherapy can be an alternate treatment option.



 XML Download
XML Download