

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Angiomyofibroblastoma (AMFB) is a rare, benign tumor of the vulva and shows a distinctive, well-circumscribed myofibroblastic feature. The tumor was firstly reported by Fletcher et al.1 in 1992. The lesion is mainly composed of conspicuous blood vessels and stromal cells. Interestingly, intralesional adipose tissue in AMFB was reported in only six cases (i.e. lipomatous variant).2
We present herein the case of lipomatous variant of AMFB in 46-year-old woman complaining of a left vulva mass.
Case Report
A 46-year-old woman, gravida 1 para 1, presented with a 2-year history of a swelling of the left vulva. The lesion had slowly increased in size. On gross examination the mass was easily movable, not adhered to adjacent tissue, and the size was 4×3×2 cm (Fig. 1A). On computed tomography (CT), highly enhanced mass was noted on the left vulva (Fig. 1B). On ultrasonogram, 4.2 cm sized subserosal myoma of the uterus and 2.2 cm sized right ovary cyst were noted. An intrauterine device was located in the uterus. No enlarged lymph node was palpated on the bilateral inguinal area. Abnormal result was not detected on laboratory test.
During the operation, there was no infiltration of tumor into deeper soft tissue and the tumor had a distinct border from the adjacent tissue. No recurrence was detected for 7 months after surgery.
1. Gross findings
The tumor was 4 cm in maximal diameter, well circumscribed, and found in the subcutis. The surgical specimen was a soft, elastic consistency without encapsulation. Neither necrosis nor hemorrhage was found. The surface had a homogeneous, glistening appearance with yellow to pinkish color (Fig. 2).
2. Microscopic findings
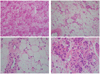
The specimen was embedded in paraffin after formalin fixation and slide sections were stained with hematoxylin and eosin. The prominent vascular pattern was noted in the mixture of hypercellular and hypocellular component. The tumor cells were aggregated in cords and nests predominantly around vessels in the edematous hypocellular matrix. The small to medium sized vessel had a dilated and thin wall. The tumor cells, round to spindle shaped, had eosinophilic cytoplasm and ovoid nuclei with uneven chromatin arrangement. No significant atypism was noted on nucleus. A lot of adipocytes with plump nucleus were scattered in the matrix (Fig. 3).
In immunohistochemistry staining, the stromal cells showed strong positivity for vimentin, estrogen receptor, and progesterone receptor. The tumor had no reactivity for desmin (Fig. 4).
DISCUSSION
AMFB occurs frequently in young-to-middle-aged premenopausal women.3,4 The tumor arises in pelviperineal subcutaneous tissue and is found predominantly in the vulva.5,6 Most of the cases exhibit painless mass of the vulva and slowly growing feature. The typical characteristics of AMFB are as follows: 1) irregular mixture of hypercellularity and hypocellularity area; 2) absence of stromal mucin.1,7
In the present case, adipose tissue was noted among the hypercellular and hypocellular area. The morphologic spectrum of AMFB is expanded to the lipomatous variant and the perivascular stem cell can be an origin of myofibroblastic and fatty differentiation.2,4,8 Only one case of lipomatous variant of AMFB was reported in men.9 A location and a size of the tumor of our case showed similar patterns, compared with 6 cases of the lipomatous variant in the literature.2 Differential diagnosis of lipomatous variant of AMFB includes Batholin's gland cyst, liposarcoma, phleomorphic sarcoma, spindle cell lipoma, aggressive angiomyxoma in vulva lesion.2,10
Because a benign condition of the vulva is very similar to that of malignancy, the primary diagnosis is very significant. Importantly, differential diagnosis is needed to rule out the aggressive angiomyxoma (AAM) in clinical situation. AAM is likely to recur locally in case of incomplete resection of the tumor.11 AMFB including lipomatous variant is frequently found at the superficial area of the vulva, while AAM infiltrates into the deeper tissue and has a greater tendency to recur.11 AMFB is well-circumscribed and not encapsulated and is generally smaller than 5 cm.7 AAM is larger than 5 cm and poorly-circumscribed.12 The stromal cells of AMFB are plump and oval shape, by comparison with that of AAM, which are spindle and stellate-shape.1,11 Once in a while, AMFB has a plasmacytoid appearance which explains a round nucleus in the plentiful cytoplasm.4,6
According to the result of immunohistochemical staining, all cases of AMFB were positive for vimentin, 92% were positive for desmin.10 It is reported that myofibroblast can be characterized by the composition of intermediate filaments protein such as vimentin and desmin.13 The strong positivity for vimentin and desmin explains a myofibroblastic origin of AFMB.10 Also, lipomatous variant of AFMB shows positivity for vimentin, ER and PR in immunohistochemistry.2 In our case, immunohistochemistry showed vimentin-positive and desmin-negative.
To our knowledge, only eight cases of AMFB have been reported in Korean literature.14 And one recurrence was described.15 It is known that the prognosis is good and local excision with clear margin is enough for the treatment.16 Our patient has no recurrence 7 months after surgery.
In conclusion, lipomatous variant of AMFB should be considered in a differential diagnosis of vulva disease and immunohistochemistry can be helpful for understanding of the disease. We herein present AMFB with adipose tissue occurring in premenopausal woman.



 XML Download
XML Download