

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Female adnexal tumors of probable wolffian origin (FATWO) were first described in 1973 by Kariminejad and Scully.1 The tumors were microscopically characterized by epithelial cells growing in diffuse, sievelike, tubular patterns. These tumors were typically located at the broad ligament where wolffian remnants are abundant, and have a different appearance to tumors of Mullerian origin.
In general, FATWOs are rare diseases and most of FATWO are benign morphological features and biological behavior. Malignant FATWOs are extremely rare neoplasms.2 There are few cases reported in the English medical literature. This is the first case reported in Korea and a malignant tumor described thus far, with distinctive morphological features being the large size of the tumor, larger than 12 cm, apparent hypercellularity, the highest mitotic activity (up to 36 /10 HPF) with demonstrable tumor implants and metastases.
We report a fortuitously discovered case of a tumor of the broad ligament having all the pathologic and clinical characteristics of a malignant FATWO displaying the highest mitotic activity.
Case Report
A 52-year-old woman, gravida 4 para 3, was referred to Cheil women's Health Care Center on May 2008 to evaluate a pelvic mass with elevated CA125 (87.8 U/mL). A pelvic examination and an ultrasound showed an 11×9×8 cm semi-solid mass containing a cystic portion at the left uterine wall, with the mass separated from the uterus. An abdomen-pelvic CT scan showed a heterogeneously-enhancing pelvic mass in close contact with the upper portion of the uterus; this tumor was thought to be a degenerating exophytic, subserosal uterine myoma. Explo-laparotomy was performed under the clinical impression of uterine myoma with second degeneration. A very large solid and yellow mass measuring 12×9×7.5 cm with suspicious infiltration of the ipsilateral salpinx was located between the right round ligament and ovarian ligament. Microscopic evaluation of a frozen biopsy revealed a FATWO with high mitotic figures (up to 36/10 HPF). A total abdominal hysterectomy and bilateral salpingo- oophorectomy, para-aortic and pelvic lymph node dissection, and omentectomy were performed. The pathologic diagnosis was malignant FATWO with tumor infiltration of the ipsilateral salpinx. There was no evidence of tumor in sections taken from 35 lymph nodes and the omentum. Adjuvant chemotherapy with three cycles of paclitaxel (175 mg/m2) and carboplatin (AUC 5) was administered. In the 10 months after adjuvant treatment, the patient has shown no evidence of recurrent or metastatic disease. Follow-up is ongoing at Cheil General Hospital and Women's Healthcare Center.
Pathologic findings
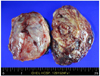
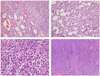
On gross examination, the tumor was well encapsulated, and the surface of the 12×9×7.5 cm solid mass was yellow-tan, smooth and glistening with focal hemorrhage (Fig. 1). Microscopically, the tumor is characterized by epithelial cells growing in various architectural patterns including tubules, cords, serve-like arrangement and solid growth. There was an eosinophilic secretion within the lumens of the cysts and tubules (Fig. 2). There was no cytoplasmic mucin product. Reticulum staining highlightened the tubular pattern. The tumor cells were cellular and slightly atypical having relatively uniform round to oval hyperchromatic nuclei and frequent mitotic activities up to 36 per 10 HPF at active areas. There was focal hemorrhage, but no necrosis. Immunohistochemical stains were positive for pan-cytokeratin, CD10 (Fig. 3), inhibin-alpha, estrogen receptor, C-kit, but negative for cytokeratin7 and cytokeratin20. Immunostaining for Ki-67 showed increased proliferation index (10~40%). The tumor invaded to salpingeal serosal wall.
Discussion
Features that appear typical of FATWO cases that have been observed to date include (a) the location that they are found, which is typically same as that of mesonephric remnants (b) their morphological dissimilarity to other ovarian tumors of either epithelial- stromal or sex cord-stromal types (c) some ultrastructural and immunohistochemical homology with the mesonephric duct (immunohistochemical evidence in support of a wolffian origin).3
In benign FATWO, the most common treatment procedure is total abdominal hysterectomy with bilateral salpingo-oophorectomy. It is unclear at this point if adjuvant chemotherapy or radiation therapy provides benefits. A patient's physical characteristics and personal preference, such as her age and desire for fertility, should certainly be considered when formulating a treatment plan.
Although most FATWO behave in a benign fashion, there have been reports of malignant tumors. It is difficult to characterize malignant tumors due to the extremely low number of reported cases. However, FATWO with high mitotic activity, cellular atypia, and necrosis generally behave in an aggressive manner.4 Furthermore, certain characteristics of malignant FATWO including hypercellularity, cellular pleomorphism, and an increased number of mitotic figures are associated with an increased risk of tumor recurrence. Our case had the highest level of mitotic figures reported to date.
It is important to examine frozen tumor sections to determine if the tumor is benign or malignant in nature, as this will determine the surgical approach that can affect the possibility of recurrence, and can also result in a drastically different prognosis. Any irregular mass discovered in a wolffian remnant location that has a different appearance to a myoma should be examined further by microscopic analysis of frozen sections. In addition to the number of mitotic figures, characteristics such as a large tumor size, increased cellularity, capsular invasion, and rupture of the capsule may predict an adverse course.5
Typically, a patient with the malignant FATWO experiences multiple recurrences and does not respond to conventional treatment. Steed et al. suggested Gleevac therapy as a targeted molecular therapy in a recurrent malignant FATWO with a c-kit-positive.3 Harada et al. also reported a FATWO that responded well to response to Gleevac treatment.4 However, in contrast to our case, the tumor in Harada et al.'s patient had a low mitotic figure. FATWO may be hormone-dependent tumors, and suggested that hormonal therapy be used in tumors with aggressive histological characteristics such as the presence of necrosis or a high mitotic index, or upon conventional treatment failure.6
In our case, the tumor was a large, malignant tumor with an unusually high number of mitotic figures that invaded the ipsilateral serosa of fallopian tube. Because of the highest mitotic figure and the tubal invasion, the patient underwent the surgical staging and three cycles of adjuvant chemotherapy.
Although the biological behavior of benign FATWO is, in general, benign, malignant FATWO's behavior is unpredictable. This report serves to remind us of the existence of female adnexal tumors of probable Wolffian origin and, in particular, their malignant potential.

 XML Download
XML Download