

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Adenomyosis was firstly used by discovered by Frankl, and pathologically defined by Bird et al. in 1972; the benign invasion of endometrium into the myometrium, producing a diffusely enlarged uterus which microscopically exhibits ectopic, non-neoplastic, endometrial glands and stroma surrounded by the hypertrophic and hyperplastic myometrium.1,2 Several previous studies were reported that the risk of adenomyosis was increased after spontaneous abortions and dilation and curettage.3,4 Uterine adenomyosis most commonly occurs in multiparous women in their late 30s or 40s, but rare in nulligravid women. Uterine adenomyosis can be classified into two categories: focal adenomyosis with lesions localized in the anterior or posterior wall; and diffuse adenomyosis with lesions in the entire uterus. Regarding obstetric problems related with adenomyosis, recent reports showed that adenomyosis was associated with infertility,5,6 spontaneous rupture of the uterus during labor in a primiparous woman,7,8 spontaneous preterm labor, preterm premature rupture of membranes (PPROM),9 and delayed postpartum hemorrhage.10 We recently experienced a case of preterm delivery at 29 gestational weeks in a primigravid woman with uterine adenomyosis.
Case Report
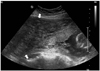
A 35-year-old woman, gravid 1 para 0 was admitted to our hospital with acute lower abdominal pain at 15th gestational week. The patient had tried unsuccessfully to become pregnant for about 2 years. In infertility work up, bilateral tubal obstruction and adenomyosis were noted. She became pregnant after undergoing in vitro fertilization and embryo transfer (IVF-ET) to be pregnant of adenomyosis. After admission, transabdominal ultrasonography (Aloka Prosound alpha-10, Tokyo, Japan) revealed uterine adenomyosis including normal gestational sac in lower uterine segment (Fig. 1). Thickened uterine wall in adenomyosis was extended from fundal area to mid portion of uterus, and in this area, there was a narrow endometrial cavity without gestational sac. Anterior wall thickness of uterus was about 10 cm, and posterior was about 3 cm. Routine chemistry, ultrasonography for exclusion of the acute appendicitis, and tococardiogram for uterine contraction was performed. Laboratory results showed hemoglobin 10.8 g/dL, white bleed cell count 20.19× 103/µL, neutrophil segmented 81%, C-reactive protein (CRP) 17.96 mg/dL (reference range: 0.01~0.3 mg/dL). With leukocytosis and elevated CRP being noted, and she had mild fever (body temperature: 37.5℃). Acute appendicitis, placental abruption, ureteral stone, and pyelonephritis were ruled out by physical examination, ultrasonography, and laboratory test. Uterine contraction was detected at 15-minutes interval. She was diagnosed with threatened abortion, and adenomyosis. She was prescribed analgesics including acetaminophen and codeine for pain control, and antibiotics with ampicillin and sulbactam were taken. Uterine contraction was subsided after hydration and bed rest. At hospital day 10, uterine cervix length estimated by transvaginal ultrasonography was 3.1 cm, abdominal pain was subsided, and she was discharged without uterine contraction.
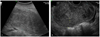
After 24th gestational week, she was repeatedly admitted to the hospital because of severe lower abdominal pain, and regular uterine contraction. Ultrasonography (Accuvix, Medison, Seoul, Korea) showed that uterine cervix was shortened and funneled (cervix length: about 1.3 cm) (Fig. 2). Tocolytics with ritodrine and analgesics including acetaminophen, codeine, nalbuphine, and pethidine were taken for uterine contraction and pain control. Pain control was daily performed due to extreme and frequent pain on low abdomen. At hospital day 6, uterine contraction was disappeared, but abdominal pain was sustained. At hospital day 9, abdominal pain was decreased, so she was discharged.
At 27th gestational week, she was readmitted with severe abdominal pain, and regular uterine contraction. Uterine cervix length estimated by transvaginal ultrasonography was 1.0 cm. In fundal area, anterior wall thickness was about 9 cm, and posterior was 3 cm. Estimated fetal weight was adequate to gestational age, but amnionic fluid index was 8 cm. There was no evidence of preterm premature rupture of membranes (PPROM). During 2 weeks, tocolytics with ritodrine and analgesics including acetaminophen, codeine, nalbuphine, and pethidine, and betamethasone were taken. At 29th gestational week, emergency cesarean section was done, because oligohydramnios (amnionic fluid index: 4), breech presentation by ultrasonography, uncontrolled abdominal pain, and fetal distress (moderate to severe variable deceleration during fetal monitoring) were noted. A male baby weighing 1,140 g was born. Apgar scores were 3 at 1 minute and 6 at 5 minute. The baby was moved to the neonatal intensive unit (NICU) with endotracheal intubation and oxygen supply. The estimated blood loss during surgery was about 500 mL. The baby had respiratory distress in the early period of NICU admission but was recovered in NICU and was discharged from the hospital after 72-day stay, and so was the mother 6-day after the operation without any other problem. Ultrasonography at 2 and 8 weeks after delivery was performed. Uterus size was serially decreased (Fig. 3).
Discussion
Because uterine adenomyosis is associated with infertility, spontaneous uterine rupture, preterm labor, and preterm premature rupture of membranes, pregnancy in a primigravid woman with uterine adenomyosis is rare and highly risky.
The effects of myoma on pregnancy or pregnancy on myoma are well known,11,12 but adenomyosis not. A recent case report showed that a rapidly growing adenomyosis was identified during the first trimester in a 35-year-old infertile woman achieving pregnancy after controlled ovarian hyperstimulation.13 Although the pregnancy was terminated at the 18th gestational week after premature rupture of membranes following genetic amniocentesis, severe abdominal pain by red degeneration was similar to our case. No imaging study for pregnant uterus for prepregnant and 1st trimester period was performed, so we don't know whether the enlarged uterine was rapidly grown during first trimester. But, pregnancy in our case was maintained to 29th gestational week, and the more the pregnancy progresses, the more severe the intensity of pain was. During follow up periods, there was no evidence of rapid growing adenomyosis. From 15th gestational to delivery, one of major problems of pregnancy maintenance was pain in our case. Various analgesics were fully used for pain control, but the pain was not satisfactorily controlled. It is well known that the most complaint associated with uterine myoma during pregnancy is pain. Although initial hypotheses suggested that pain was secondary to fibroid growth during pregnancy, painful episodes appear to be unrelated to absolute fibroid size or growth.14 Prospective, longitudinal studies have also failed to document significant change in fibroid size during pregnancy.15-17 A case for successful pregnancy outcome in a woman with large uterine intramural myoma was reported by Skrablin S et al. Pregnancy with about 13 cm sized intramural myoma in fundal area was reported. That case showed that abdominal pain did not worsen during pregnancy, and an elective cesarean section was performed at 38 weeks.18 However, it is little known that pregnancy with adenomyosis is associated with pain. The most common cause of neonatal morbidity reported in any of these studies was preterm delivery. Women with myomas in pregnancy seem to be at increased risk of threatened preterm labor with reported rates of up to 21.5%, and the risk of preterm labor correlated positively with the size of the largest fibroid. And it is generally accepted that tocolytic agents used in pregnancy with myoma and preterm labor is not different from with only preterm labor.19-22
In this case, the pregnant woman had low abdominal pain, mild fever, leukocytosis, and increased inflammatory markers. These symptoms and signs were similar to that of pregnancy with red degeneration of myoma. Also, it was difficult to differentiate the pregnancy with uterine adenomyosis from other medico- surgical, and obstetrical problems such as appendicitis, placental abruption, preterm labor, ureteral stone, pyelonephritis, and chorioamnionitis.
Here, we report the case of preterm delivery accompanied by various complications such as uncontrolled pain, preterm labor, and oligohydramnios in a woman with uterine adenomyosis.

 XML Download
XML Download