

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
About 20~30% of benign or malignant tumors of ovarian origin arise from embryonic cells, and only 3% represent malignancy. But under age of 20, 70% of ovarian tumors arise from embryonic cells, and over 1/3 of them are malignant tumors. Over all the ovarian tumors arising from embryonic cells, immature teratoma is germ cell tumor, components include immature tissues and cells derived from ectoderm, mesoderm, and endomermal origins. Most of the immature tissues are from neuroectodermal origins. The immature teratoma of the ovary is a rare tumor, representing less than 1% of all ovarian neoplasm. These tumors typically present in young age woman (mean age 10~20 years) with pelvic and abdominal pain. Nowadays newly developed combination chemotherapeutic agents such as bleomycin, etoposide, cisplatin give us great survival and disease free prognosis than before. We have experienced two cases of immature teratoma so we report them with a brief review of concerned literatures.
Figures and Tables
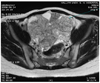
Fig. 1
On pelvis magnetic resonance imaging, there is about 20×10×18 cm sized large cystic and solid component possesing fatty mass.

Fig. 2
The resected ovary. The external capsule of ovarian mass is smooth and glistening. The mass in predominantly solid, fleshy, and gray-tan cystic with mucinous fluid.

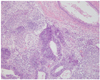
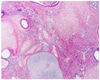
Fig. 4
On pelvis magnetic resonance imaging, there is about 15×10×20 cm sized large lobulated mass, mostly solid component. It shows numerous internal cacification.

References
1. Scully RE, Young RH, Clement PB. Tumors of the ovary, maldeveloped gonads, fallopian tube, and broad ligament: atlas of tumor pathology (Afip atlas of tumor pathology No. 23). 1998. Washington: Armed Forces Institute of Pathology.
2. Norris HJ, Zirkin HJ, Benson WL. Immature (malignant) teratoma of the ovary: a clinical and pathologic study of 58 cases. Cancer. 1976. 37:2359–2372.
3. Taylor CW, Haines M, Fox H. Haines and Taylor obstetrical and gynecological pathology. 1987. 3rd ed. Edinburgh: Churchill Livingstone.
4. Curry SL, Smith JP, Gallagher HS. Malignant teratoma of the ovary: prognostic factors and treament. Am J Obstet Gynecol. 1978. 131:845–849.
5. Nogales FF Jr, Ortega I, Rivera F, Armas JR. Metanephrogenic tissue in immature ovarian teratoma. Am J Surg Pathol. 1980. 4:297–299.
6. Kawai M, Furuhashi Y, Kano T, Misawa T, Nakashima N, Hattori S, et al. Alpha-fetoprotein in malignant germ cell tumors of the ovary. Gynecol Oncol. 1990. 39:160–166.
7. Berek JS, Fu YS, Hacker NF. Berek JS, Adashi EY, Hillard PA, editors. Ovarian cancer. Novak's Gynecology. 1996. 12th ed. Baltimore: Williams & Wilkins;1201.
8. Robboy SJ, Scully RE. Ovarian teratoma with glial implants on the peritoneum. An analysis of 12 cases. Hum Pathol. 1970. 1:643–653.
9. Fortt RW, Mathie IK. Gliomatosis perionei caused by ovarian teratoma. J Clin Pathol. 1969. 22:348–353.
10. Norris HT, O'Conner DM. Coppleson M, editor. Pathology of malignant germ cell tumors of the ovary. Gynecologic oncology. 1992. 2nd ed. New York: Churchill Livingston;917–934.
11. Slayton RE. Management of germ cell and stromal tumors of the ovary. Semin Oncol. 1984. 11:299–313.
12. Kawai M, Kano T. Seven tumor markers in benign and malignant germ cell tumors of the ovary. Gynecol Oncol. 1992. 45:248–253.
13. Jung MH, Kim DY, Kim JH, Kim YM, Kim YT, Nam JH, et al. Clinical anapysis of 24 cases of immature teratoma of the ovary. Korean J Obstet Gynecol. 2005. 48:2926–2931.
 XML Download
XML Download