

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of renal cell carcinoma is consistently increasing, and the increase in use of imaging technologies has resulted in an increase in the incidental detection of renal cell carcinoma, especially of small renal masses [1]. Nephron-sparing surgery has become the standard treatment for small renal masses, demonstrating improved overall survival and superior preservation of renal function compared with traditional radical nephrectomy [2]. In addition, laparoscopic partial nephrectomy (LPN) and robot-assisted partial nephrectomy (RPN) have been accepted as treatment options for small renal masses with adequate oncologic outcomes [3].
Several factors predict renal functional outcome after partial nephrectomy, including older age, sex, lower preoperative glomerular filtration rate (GFR), single kidney, tumor size, and longer ischemic interval [4]. The warm ischemia inevitable in LPN or RPN can produce ischemic renal damage. The limit of 30 minutes in patients with normal preoperative kidney function is currently accepted as a safe warm ischemia time (WIT) [56]. Our previous study demonstrated that patients with a WIT>28 minutes had a significantly greater decrease in the GFR of the affected kidney; in multivariate analysis, WIT was an independent predictive factor of functional reduction of the affected kidney [7]. Although a WIT ranging from 20 to 30 minutes was thought to be safe, some authors have suggested that every minute counts when the renal hilum is clamped. To minimize ischemic renal injury, many surgeons make an effort to decrease the WIT to less than 30 minutes during partial nephrectomy under pneumoperitoneum. However, there are few studies on preoperative predictors of prolonged WIT during LPN or RPN performed by a single surgeon. In this study, we evaluated patients who underwent LPN or RPN and tumor characteristics predictive of prolonged WIT.
MATERIALS AND METHODS
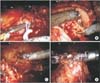
With the approval of our Institutional Review Board, we retrospectively analyzed the medical records of 317 patients who underwent partial nephrectomy. Partial nephrectomy was conducted by laparoscopic or robot-assisted surgeries and was performed by the same surgeon between October 2007 and May 2013. According to the tumor location, we performed transperitoneal approaches for anteriorly or laterally located tumors and retroperitoneal approaches for posteriorly located tumors. For arterial clamping during surgery, we used Bulldog clamps (Aesculap, Center Valley, PA, USA) (Fig. 1A). Color Doppler laparoscopic ultrasound was used to confirm whether hilar clamping was proper or not. Resection of the tumor was completed with scissors, without application of electrosurgical coagulation devices (Fig. 1B). After tumor excision, surgical bed hemostasis was achieved by oversewing vessels by using 3-0 PDS or 3-0 V-Loc sutures with a Lapra-Ty clip (Ethicon, Cincinnati, OH, USA) at the terminal end (Fig. 1C). The renal parenchyma was repaired with 1-0 Vicryl sutures placed in an contiuous fashion across the defect, and the sliding technique with Hem-o-lok clip was used to tighten and secure the sutures (Fig. 1D). Our surgical technique is demonstrated in a Supplementary material (video clip). Ischemia time was defined as the interval between placement of the first arterial clamp and removal of the last clamp.
Demographic and patient characteristics were recorded, including age, sex, body mass index, American Society of Anesthesiologists classification, preoperative estimated GFR, clinical tumor size, and pathologic outcome. Clinical tumor size was recorded as the largest diameter seen on radiological images. The nephrometry score (nephrometry score; R.E.N.A.L. [radius, exophytic/endophytic, nearness to collecting system or sinus, anterior/posterior and location relative to polar lines] score, PADUA [preoperative aspects and dimensions used for an anatomical] score, and C-index) was determined by a retrospective review of images. Patients were divided into two groups: group A was defined as prolonged WIT (≥30 minutes) and group B as short WIT (<30 minutes). Patient characteristics were compared between the two groups.
Perioperative outcomes including operative time, estimated blood loss (EBL), pathologic tumor size, method of surgery (LPN or RPN), and approach method (transperitoneal or retroperitoneal) were compared between groups. We evaluated multiple factors as predictors of prolonged ischemic time. To assess the impact of surgeon experience on WIT, we categorized the patients in groups of 50 consecutive cases.
All data analyses were performed by using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA) and SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Student t-tests and Pearson chi-square tests were used for comparisons of means and proportions, respectively. Univariable and multivariable regression models were used to assess predictors of intraoperative prolonged WIT. All tests were two-sided, and statistical significance was set at p<0.05.
RESULTS
Among the 317 consecutive patients, there were 209 males (65.8%) and 108 females (34.2%) with a median age of 53.5 years (range, 29-78 years). A total of 80 patients were included in group A and 237 patients in group B. Mean WIT was 38.6±8.9 minutes in group A and 19.8±5.8 minutes in group B, respectively (Table 1).
Demographic characteristics were not significantly different between the two groups. However, the PADUA score (p=0.006), R.E.N.A.L. score (p=0.003), operative time (p<0.001), EBL (p<0.001), and approach method (p<0.001) did differ significantly between the two groups (Table 1).
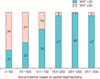
Concerning surgeon experience, the group proportions changed over time. Cases 1-50 (group A: 68% vs. group B: 32%) and 51-100 (group A: 54% vs. group B: 46%) had higher proportions of group A than group B. After these 100 cases, WIT significantly decreased, ultimately demonstrating an absolute majority of patients in group B after the surgeon had accumulated more than 150 cases (p<0.001) (Fig. 2).
Univariable analysis identified PADUA score (p=0.008), approach method (<0.001), and surgeon experience (p<0.001) to be significantly associated with prolonged WIT. In the multivariable analysis, PADUA score (p=0.032), tumor size (odds ratio [OR], 2.98; 95% confidence interval [CI], 1.48-5.96; p=0.002), and surgeon experience (p<0.001) were independent predictors of prolonged WIT. Among these, surgeon experience was the strongest independent predictor. According to cumulative surgery cases, compared with the experience of 50 cases of surgery, although the risk of prolonged WIT was not reduced from cases 51-100 (p=0.202), as subsequent surgery experience accumulated, a significant reduction in prolonged WIT was shown (Table 2).
In a subanalysis according to type of surgery (RPN or LPN), tumor size (OR, 3.21; 95% CI, 1.24-8.28; p=0.016) and surgeon experience (p<0.001) were independent predictors of prolonged WIT in the RPN group, whereas surgeon experience (p<0.001) was the only independent predictor of prolonged WIT in the LPN group (Table 3). Among the variables making up the nephrometry score, the R.E.N.A.L. score in patients who underwent RPN (6.75±1.42) was higher than that of those who underwent LPN (5.96±1.48, p<0.001).
DISCUSSION
Current guidelines show that patients with clinically staged T1 renal tumors should undergo partial nephrectomy whenever technically feasible [8]. Several retrospective studies have shown acceptable oncologic outcomes of partial nephrectomy for not only small renal tumors, but also large localized renal tumors [910]. Postoperative renal function is better preserved with partial nephrectomy than with radical nephrectomy; however, several clinical factors impact renal function after surgery, and profound renal functional loss can occur even after partial nephrectomy. Since Lane et al. [4] showed that ischemia time during partial nephrectomy is the greatest modifiable predictive risk factor of postoperative functional loss, WIT has been found to be associated with a significant loss of renal function of the affected kidney, mainly in patients who experienced prolonged WIT. To date, however, there are few studies on factors that affect WIT prolongation.
In the comparison of perioperative factors between groups A and B, the ratios of the surgical approach method differed. This finding is attributed to the fact that the transperitoneal approach was used in a large proportion of the initial cases in our series. As surgical experience accumulated, the surgeon's preference changed to a retroperitoneal approach for posterior or laterally located renal tumors. Actually, surgical approach was not a predictor of WIT, as shown by the multivariable analysis.
There are several reports of a higher nephrometry score being significantly associated with increased WIT [111213]. Ficarra et al. [12] found that surgeon experience, clinical tumor size, anatomic characteristics determined by the PADUA classification score, and upper collecting system repair were independent predictors of WIT>20 minutes. Recently, Wang et al. [13] showed a much stronger correlation between nephrometry score and WIT, with the C-index system (coefficient, -0.609) and the PADUA score system (coefficient, 0.735) showing the strongest correlation in the overall analysis, whereas the R.E.N.A.L. nephrometry score showed a relatively weaker correlation. In concordance with previous studies, our results indicate that each component of the nephrometry score is correlated with WIT. Among the variables making up the nephrometry score, our study demonstrated that only the PADUA score (p=0.032) could predict WIT>30 minutes. These findings suggest that risk group stratification using the PADUA score may improve patient selection for partial nephrectomy, especially for novice surgeons.
However, the results of our subgroup analysis showed that using the nephrometry score to predict prolonged WIT in the groups divided by surgical type (RPN or LPN) was not effective. We hypothesize that this discrepancy in results depends on the WIT cutoff value. Previous studies have set the WIT cutoff value to 20 minutes, whereas we evaluated the predictors of prolonged WIT defined as longer than 30 minutes.
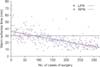
Regarding surgeon experience, Mottrie et al. [14] demonstrated that surgeon experience significantly correlated with robotic console time (p<0.001) and WIT (p<0.0001). We also found that surgeon experience was associated with reduced risk of prolonged WIT. We stratified the cases into six chronologic periods of 50 accumulative cases. When we compared each period, the ratios of group A were 68%, 54%, 30%, 6%, 4%, and 4%, respectively. Our data showed that prolonged WIT was very rare when surgeon experience was greater than 150 cases of partial nephrectomy under pneumoperitoneum. In further subgroup analysis, surgeon experience was the most important predictor of WIT in both the RPN and LPN groups. After 50 cases of each type of surgery were accumulated, the risk of prolonged WIT was reduced dramatically compared with that in the first 50 cases (Fig. 3).
Several current studies have shown shorter learning curves for RPN than for LPN. Two systematic reviews and meta-analyses of RPN versus LPN reported no significant differences in perioperative outcomes between the two groups, except for a significantly shorter WIT [1516]. However, type of surgery was not predictive of prolonged WIT in the present study. Several possible confounding factors could have impacted this result. More complex cases were treated with RPN because of its likelihood to greatly mitigate the difficulty of complex partial nephrectomy.
CONCLUSIONS
Surgeon experience, PADUA score, and tumor size are significant predictors of prolonged WIT during partial nephrectomy under pneumoperitoneum. Among these predictive factors, accumulating surgical experience is the most important and the only modifiable factor for reducing the risk of prolonged WIT.




 XML Download
XML Download