

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Incidental detection of small renal masses is increasing. This has led to an increase in biopsy of small renal masses, a proportion of which are then proven to be benign. Needle biopsy of small renal masses is controversial owing to the risk of seeding malignant cells along the needle tract. Needle tract seeding is a rare event; the incidence is estimated to be less than 1 in 10,000 cases of all biopsies [1]. Eight other cases of needle tract seeding in a renal mass biopsy have been described in the medical literature, two as recently as 2013 (Table 1). Complications in these patients include distant metastasis and death. We report our experience of a man with renal cell carcinoma (RCC) seeding along a biopsy tract and compare the circumstances and biopsy techniques with reported cases in the literature.
CASE REPORT
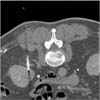
A 66-year-old man was incidentally found to have a 32-mm right lower pole renal mass on a computed tomography (CT) scan (Fig. 1). CT-guided needle biopsy of the renal mass (Fig. 2) revealed Fuhrman grade 2 clear cell RCC. Two samples were obtained by use of a 16-gauge Temno core biopsy needle (CareFusion, San Diego, CA, USA) and a 22-gauge Francine needle. One pass was made for each needle sampling. No coaxial needle was used. Within 2 months, the patient underwent right partial nephrectomy. Perinephric fat was sent along with the excised renal lesion for histopathological analysis. No specific feature of tumor seeding was seen intraoperatively. Histopathology revealed a well-circumscribed 30-mm clear cell RCC, predominantly Fuhrman grade 2 with focal areas of grade 3. There was an area where the capsule was interrupted that corresponded to a hemorrhagic area on the cortical surface (Fig. 3). A tumor deposit was also noted in the perinephric fat. These features suggested that the tumor deposit in the fat was likely due to tumor seeding rather than a metastasis and that the tumor seeding could have resulted from the needle biopsy. His TNM staging was pT3a NX MX, at least stage 3 disease (American Joint Committee on Cancer, 7th edition, 2010) and his Leibovich score was 5 (intermediate risk). Six months after the operation, there was no radiological evidence of tumour recurrence on a CT scan.
DISCUSSION
Aside from the potential for false-negative results, a key risk of renal mass biopsy is seeding of the biopsy tract with malignant cells. Several factors in theory could affect the risk of biopsy tract seeding, such as needle size, the number of needle passes, and the use of a coaxial needle. Biopsy tract seeding has been reported in renal mass biopsies using needles as fine as 23-gauge and as large as 14-gauge [234]. Theoretically, a larger-bore needle would increase the risk of seeding owing to an increased area of defect on the surface of the tumor and an increased circumference or surface area of the needle. However, because of the scarcity of cases, it is difficult at this stage to accurately determine a relationship between needle size and the risk of seeding. It is also difficult because of underreporting to associate the risk of needle tract seeding with the number of needle passes through a tumor.
Use of a coaxial needle allows multiple passes through the renal mass with only one pass through the surrounding normal tissue. This theoretically reduces the risk of needle tract seeding into normal tissue and potentially reduces patient discomfort as well [5]. Although it is interesting to note that a coaxial needle was not used in any of the currently reported cases of needle tract seeding after renal mass biopsy (Table 1), there are just too few cases to establish a firm relationship between the risk of biopsy tract seeding and the use of a coaxial needle. Visualization of larger coaxial needles on ultrasound or CT may be easier than with smaller biopsy needles [5], and this may improve accuracy.
Histological evidence of biopsy tract seeding may not always be found after definitive surgery to remove the renal mass. Seeding into excised perinephric tissues can be found soon after surgery but seeding into surrounding muscle, fascia, and skin may only be apparent months, or even years, after surgery. As was seen with this case, the biopsy needle traversed skin, subcutaneous tissue, multiple muscle and fascia layers, and perinephric fat before reaching the renal lesion (Fig. 2). Thus, the tumor could theoretically seed into one or more of these tissues; seeding as superficial as the subcutaneous tissue has been reported (Table 1). This delayed presentation may increase the risk of adverse outcomes such as further metastasis and poorer prognosis. Time to presentation or diagnosis of tumor seeding after renal mass biopsy has ranged from 24 days to 84 months in previously reported cases where tumor seeding was not found on the initial histopathological analysis (Table 1).
In conclusion, a common feature in all reported cases of needle tract seeding from a renal mass biopsy is that a coaxial needle was not used. However, because of the paucity of cases, there is currently no satisfactory association between the risk of needle tract seeding and needle size or the number of needle passes. It is important to consider that histopathological evidence of needle tract seeding may not be apparent in all cases, especially if seeding occurred beyond the excised tissues.



 XML Download
XML Download