

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Daily use of selective serotonin reuptake inhibitors (SSRIs) very effectively delays ejaculation in men with lifelong premature ejaculation (PE) [1]. Compared to the other SSRIs, daily use of 20-mg paroxetine hemihydrate exerts the strongest ejaculation delay [1]. However, this is not always the case. The extent of ejaculation delay differs between men. For example, in a stopwatch study of 54 men with lifelong PE that investigated the association between paroxetine-induced ejaculation delay and the 5-HTTLPR polymorphism [2], 43 men (80%) responded with an ejaculation delay, whereas 11 (20%) did not. A similar result was found by Salonia et al. [3] in a group of 65 men with lifelong PE with an estimated intravaginal ejaculatory latency time (IELT) of less than 1 minute. Of these patients, 15 men (23%) discontinued daily paroxetine treatment within 3 months because the ejaculation delay was below expectation, e.g., paroxetine had a minimal ejaculation delaying effect [3].
In rather rare cases, men with lifelong PE do not respond to any SSRI treatment with an ejaculation delay. This phenomenon has so far not been mentioned in the literature of PE and has never been investigated. Theoretically, ultraextensive metabolizers of paroxetine may not respond with an ejaculation delay because an adequate paroxetine concentration may not be established [4]. Apart from this potential pharmacokinetic factor, animal studies have also shown that pharmacodynamic factors, such as the amount of serotonin neurotransmission and/or 5-HT1A receptor activation, are associated with the extent of ejaculation delay [5,6]. However, whether pharmacokinetic or pharmacodynamic factors may explain the (nearly) complete absence of SSRI-induced ejaculation delay in some men with lifelong PE remains unknown. It is of note that SSRI-induced ejaculation delay has been suggested to be related to decreased serum leptin levels [7] and that there is a relationship between serum plasma testosterone levels and the serum leptin level [8].
The aim of the current study was to investigate the role of various pharmacokinetic factors (e.g., paroxetine dosage, serum paroxetine level, Cyp2D6 activity) and serum leptin, gonadotrophin, and prolactin levels, all of which had previously been suggested to be related to PE and SSRI-induced ejaculation delay [7,9,10]. In addition, on the basis of the hypothesis of Waldinger et al. [11] that the IELT in men with lifelong PE is related to 5-HT1A and/or 5-HT2C receptor functioning, we investigated the role of 5-HT1A receptor gene C(-1019)G polymorphism. Owing to the rarity of the phenomenon, a small number of patients and controls was inevitable and necessitated a strict protocol of procedures and interventions.
MATERIALS AND METHODS
1. Patients
Included were patients with complaints of lifelong PE. As (nearly) complete absence of any paroxetine-induced ejaculation delay together with absence of ejaculation delay after another serotonergic antidepressant is an infrequent clinical phenomenon as far as we know, we informed 5 males who had been (unsuccessfully) treated by the last author before the start of the current study about the purpose of the study. All of these patients agreed to participate in the current study, which meant that they could not take an SSRI or clomipramine for 6 months prior to the start of the study. On the other hand, we recruited 8 new patients with lifelong PE who after telephone screening were seen at the Outpatient Department of Neurosexology of Haga Hospital in the Netherlands. All men were informed about the purpose of the current study, which was to investigate factors that may contribute to paroxetine-induced ejaculation delay.
All patients included were heterosexual men aged 18 to 65 years with lifelong PE. All patients had a stable relationship with a female partner. Exclusion criteria were erectile dysfunction, alcohol or substance abuse, mental disorders, physical illnesses, concomitant medications, a history of sexual abuse, serious relationship problems, a history of very low intercourse frequency, pregnancy of the partner or pregnancy wish in the near future, and possible unacceptable risks for occupational hazards owing to side effects of the study drugs.
Informed consent was obtained from all patients after the study and possible side effects were explained. The study was approved by the Hospital Medical Ethical Committee and was conducted in accordance with the Helsinki Declaration of 1975 as revised in 1983.
2. Assessment and treatment
Lifelong PE was defined according to the International Society for Sexual Medicine (ISSM), e.g., a male sexual dysfunction characterized by ejaculation which always or nearly always occurs prior to or within about 1 minute of vaginal penetration, and the inability to delay ejaculation on all or nearly all vaginal penetrations, and negative personal consequences, such as distress, bother, frustration, and/or the avoidance of sexual intimacy [12].
The IELT was defined as the time between the start of vaginal intromission and the start of intravaginal ejaculation [13]. Because a placebo response to SSRI-induced ejaculation delay has been shown to be less than two folds the increase of the geometric mean IELT [1], response to treatment in the current study was defined as a fold increase (FI) of the geometric mean IELT higher than 2 (FI=IELT value at the end of treatment period/IELT value at baseline).
Patients attended the outpatient department approximately 1 month before the start of treatment (first baseline assessment), on the day before treatment (second baseline assessment), and at the end of three consecutive series of 4 weeks of daily treatment with 10-, 20-, and 30-mg paroxetine, respectively.
At the first visit, patients were interviewed individually by the last author and asked for an independent estimation of the IELT. A stopwatch and instructions on how to measure the IELT with the stopwatch were provided. The IELT was measured at home over the following 16 weeks. The female partners had to handle the stopwatch. Patients were instructed not to have interrupted intromission or to increase their speed of intercourse. This instruction was checked during later visits to the clinic. If intercourse took place more than once at the time of IELT measurement, only the first episode of vaginal penetration with ejaculation was included. Patients were not permitted to use condoms or topical anaesthetics during the study, and no psychotherapeutic interventions were made.
After a 1-month baseline period, patients received half tablets of paroxetine hydrochloride hemihydrate 20 mg for 4 weeks. The study medication was provided by the Hospital Pharmacy Department. The patients were requested to take half a tablet (10 mg) once daily in the morning in the first month of treatment and one tablet (20 mg) daily in the morning in the following 4 weeks. In the last month, the patients took 1 tablet of paroxetine 30 mg daily in the morning. After each period of 4 weeks, patients returned to the hospital. On that day, blood samples of leptin and paroxetine were taken at 4 fixed times in the morning, e.g., at 8:30 AM, 9:30 AM, 10:30 AM, and 11:30 AM, respectively. At 9:00 AM one tablet of 10-, 20-, or 30-mg paroxetine was taken during the first, second, and third month, respectively. At the time of blood sampling and paroxetine intake, the patients were sober and had fasted for 12 hours. Peripheral venous blood samples were taken by the first author.
3. Laboratory analysis
1) Leptin concentrations
Serum leptin concentrations were assessed with a validated method of analysis (Human Leptin RIA kit [250 tubes]; catalog #HL-81K; Human Linco Research Inc., St. Charles, MO, USA) with a lower limit of quantification of 0.5 ng/mL and a variation coefficient that was dependent on the serum leptin concentration [8]: 8.3% at 4.9 ng/mL, 4.6% at 7.2 ng/mL, and 3.6% at 25.6 ng/mL.
2) Paroxetine concentrations
Serum paroxetine concentrations were assessed with a validated method of analysis with a lower limit of quantification of 3.7 µg/L and a variation coefficient of 2.9%. Because the concentration of paroxetine is dependent on its metabolism, it should be noted that the metabolism of paroxetine has a linear and a nonlinear component [14]. The nonlinear component is caused by transversion of paroxetine by CYP2D6. CYP2D6 has been investigated on the presence of mutations *3, *4, and *6. The CYP2D6*3, *4, and *6 mutations are coding for enzymes that are less active than the (wildtype) enzymes [14]. Genotyping of the CYP2D6 enzymes was performed by Taqman analysis. Of the CYP2D6 mutations, the *3, *4, and *6 mutations are most frequently seen in Caucasians [14]. More than 95% of slow metabolizers in a Caucasian population can be determined by assessing these mutations [4].
3) 5-HT1A receptor gene polymorphism (C-1019G)
For a 50-µL polymerase chain reaction (PCR), we used about 10 ng of genomic DNA. The primers of the 5-HT1A receptor gene polymorphism (C-1019G) were as follows: P1 (5'-GGC TGG ACT GTT AGA TGA TAA CG-3') and P2 (5'-GGA AGA AGA CCG AGT GTG TCA T-3'). The underlined nucleotide is a mismatch with the 5HT sequence, creating a restriction site in the PCR product. PCR conditions were as follows: 7 minutes at 94℃; 35 cycles of 1 minute at 94℃, 1 minute at 59℃, and 1 minute at 72℃; and finally 7 minutes at 72℃. The size of the amplified product was 163 bp. Then the PCR product (10 µL) was digested with BseGII (Fermentas) in a total volume of 15 µL for 1 hour at 55℃ and subsequently analyzed on a 3% agarose/Tris-borate-ethylenediaminetetraacetic acid gel with ethidium bromide staining. The fragment obtained for the wild-type allele was 163 bp and those for the variant allele were 146 and 17 bp.
4. Statistical analysis
Data analysis was performed with IBM SPSS Statistics ver. 19.0 (IBM Co., Armonk, NY, USA). Student t-test was performed for the comparison of various concentrations of leptin and paroxetine. Regression analysis was performed to assess the alterations of leptin concentrations during the day and throughout the 16 weeks of the current study. Differences were considered significant at p<0.05.
RESULTS
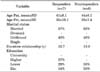
The characteristics of the patients are shown in Table 1. The study included 6 paroxetine nonresponders and 7 responders. Notably, one of these nonresponders was among the newly recruited men. Because this individual only appeared to not respond to daily paroxetine treatment, he differed from the 5 previously known men who did not respond to paroxetine and another SSRI or clomipramine. No significant differences were found between the groups in age, marital status, or duration of relationship.
Table 2 shows the baseline IELT values, the FIs of the geometric mean IELT after the three paroxetine treatment periods, and the body mass index (BMI) at baseline and at the end of the study. The IELTs were not significantly different between the responders and the nonresponders at baseline. All 6 paroxetine nonresponders had a FI of less than 2, ranging from 1.1 to 1.7. In contrast, the 7 paroxetine responders had a FI of more than 2, ranging from 2 to 8.8 in relation to the dosage of paroxetine treatment. The number of intercourses at baseline in the responder and nonresponder groups was 7 and 5, respectively. In the three drug treatment periods, the number of intercourses was 5, 4, and 4 in the responders and 6, 5, and 5 in the nonresponders, respectively.
In the responders, the FI of the geometric mean IELT during the three paroxetine treatment periods was significantly different between the 10-, 20-, and 30-mg doses (p=0.004) and between the 20- and 30-mg doses (p=0.049). In the nonresponders, the FI of the geometric mean IELT during the three paroxetine treatments periods was not significantly different, e.g., 10 mg versus 20 mg (p=0.43) and 20 mg versus 30 mg (p=0.11). Between responders and nonresponders, the FI in the geometric mean IELT was significantly different after 10-mg (p=0.003), 20-mg (p=0.002), and 30-mg (p=0.026), respectively.
BMI at baseline and at the end of study was not significantly different in the responders and nonresponders (p=0.49).
The serum leptin levels at baseline at 8:30 AM and at 9:30 AM, 10:30 AM, and 11:30 AM and after each month of treatment with 10-, 20-, and 30-mg paroxetine are shown in Table 3. Serum leptin levels at baseline were similar in the responders and nonresponders, and during the three paroxetine treatment periods they were not significantly different compared with their baseline values. The serum leptin level during the 10-mg paroxetine period was not significantly different from baseline (p=0.20), neither was the level during the 20-mg (p=0.30) or 30-mg (p=0.31) period. Moreover, serum leptin levels were not significantly different between responders and nonresponders (p=0.42).
The serum paroxetine concentrations at 8:30 AM, 9:30 AM, 10:30 AM, and 11:30 AM after each month of treatment with 10-, 20-, and 30-mg of paroxetine are shown in Table 3. In the responders, serum paroxetine concentrations increased between the 10- and 20-mg doses (p=0.023), between the 20- and 30-mg doses (p=0.095), and between the 10- and 30-mg doses (p=0.014). In the nonresponders, serum paroxetine concentrations increased between the 10- and 20-mg doses (p=0.064), between the 20- and 30-mg doses (p=0.034), and between the 10- and 30-mg doses (p=0.025). Between the responders and nonresponders, no significant differences were seen between the 10-mg (p=0.45), the 20-mg (p=0.33), and the 30-mg dose (p=0.17).
No association was found between the FI in the geometric mean IELT and serum paroxetine levels during the three treatment periods, (y=0.1035x + 2.9411/R2=0.066) (Fig. 1). Moreover, no association was found between leptin levels during the treatment periods and paroxetine serum levels.
Genetic research showed that all nonresponders to paroxetine treatment were heterozygote (GC genotype) for the 5-HT1A receptor C-1019G variation. In contrast, all paroxetine responders had the wildtype (CC) genotype for the 5-HT1A receptor C-1019 G variation (Fig. 2).
Table 4 shows the serum concentrations of testosterone, luteinizing hormone, follicle stimulating hormone, sex hormone binding globuline, prolactin, thyroid-stimulating hormone (TSH), and T4-free at baseline and at the end of 8 weeks of paroxetine treatment in both the paroxetine responders and nonresponders. The table shows that within both groups, treatment did not result in significant changes in serum concentrations. However, it is remarkable that serum prolactin levels increased during treatment in the responder group, whereas serum prolactin levels tended to decrease during treatment in the nonresponder group. This change in serum prolactin concentrations is represented in Fig. 3. The difference in the change in the serum prolactin level in the responder group compared with the change in the nonresponder group was statistically significant (p=0.044). However, although this phenomenon suggests an association between prolactin release and paroxetine treatment response and perhaps with central 5-HT metabolism, it should not be considered in terms of a causal relationship because this remains unclear.
DISCUSSION
Given that complete nonresponse to paroxetine and another SSRI or clomipramine is rare, we were only able to include 5 nonresponders who had been unsuccessfully treated at our outpatient department in the previous 2.6 (standard deviation, ±3.6) years with paroxetine 20-30 mg/d, sertraline (n=3), on-demand use of clomipramine (n=2), eutectic mixture of local anesthetics crème (n=3), and tramadol (n=1). Because one of the newly recruited men also showed no response to paroxetine treatment, we decided after the end of the study to include this man in the nonresponder group. Therefore, the current study involved 7 responders and 6 nonresponders to daily paroxetine treatment.
A clear dose-effect relationship was found in the responder group, with the highest FI (8.8) of the geometric mean IELT in men using 30-mg paroxetine compared with those using 10-mg paroxetine (FI, 2.0). At baseline (e.g., 8:30 AM) the serum concentrations of paroxetine in both the responders and the nonresponders were similar at the start of paroxetine treatment. In both the responders and the nonresponders, the serum concentration of paroxetine increased with increasing dosage. No significant differences in serum levels at the different dosages of paroxetine were found throughout the whole period of study between the responders and nonresponders. Therefore, it may be concluded that in the nonresponders, increasing serum levels of paroxetine did not result in a clinically relevant ejaculation delay even though the serum paroxetine levels were similar between the responders and nonresponders.
Notably, because serum levels of leptin were not associated with the three different dosages of paroxetine, and remained similar in the responders and nonresponders throughout the whole study period, it may also be concluded that the paroxetine-induced ejaculation delay was not associated with the serum leptin level. In this respect, it should be emphasized that at baseline, serum leptin levels were similar in responders and nonresponders and were within the normal range (3.8±1.8 ng/mL) of males with a BMI of 18 to 25 kg/m2 [14]. Notably, the BMI of both the responders and the nonresponders was similar at baseline and at the end of the study.
Importantly, in both responders and nonresponders, the serum leptin level was not associated with the serum paroxetine level and did not show any association with the FI of the geometric mean IELT.
In the current study, Cyp2D6 genotypes were investigated by measuring *3, *4, *6 and ultraextensive metabolism. There were no patients with ultraextensive metabolism. The majority of men had the Cyp2D6*1 mutation (homozygote wildtype), but there were two men with the Cyp2D6 *3 and *4 mutations, respectively. In other words, in these men there is less Cyp2D6 activity, which may result in higher paroxetine plasma levels. Indeed, it was found that while using 30 mg of paroxetine per day, these men had a higher serum paroxetine level than did men without these Cyp2D6 mutations. However, because the number of patients was low, we cannot make any conclusions about the significance of this higher paroxetine level in relation to these mutations. Moreover, the IELTs of these men were not significantly different, and the BMI and the serum leptin level also did not differ significantly compared with values in men without the Cyp2D6 mutation. In other words, the IELT in these men was not dependent on the serum paroxetine level, the serum leptin level, or BMI.
Interestingly, we found that the 6 paroxetine nonresponders were heterozygous (GC genotype) for the 5-HT1A receptor C-1019G variation, whereas the 7 responders had the wildtype (CC) genotype. However, note that these findings could be the result of a selection bias, because before the onset of the study, we purposely selected 5 nonresponders to previous paroxetine and other SSRI and clomipramine treatment. Intriguingly, although the number of patients in both groups was very low, a similar finding in responders and nonresponders was not present in our previous study investigating the 5-HTTLPR polymorphism and paroxetine-induced ejaculation delay in 54 men with lifelong PE, in which nonresponse to paroxetine-induced ejaculation delay was present in 20% of men [2]. Because the 5-HT1A receptor is important in mediating ejaculation, the current finding warrants further research of this phenomenon in larger group of men with lifelong PE.
Apart from the aforementioned difference in 5-HT1A receptor gene polymorphism in paroxetine responders and nonresponders, the current study shows another interesting difference between the groups. The serum prolactin level increased in the responders, whereas it tended to decrease in the nonresponders. Although the prolactin increase in the responders was not significantly different compared with the baseline values in the responder group, and the prolactin decrease in the nonresponders was not significantly different compared with the baseline values in the nonresponder group, the change (+delta) in the prolactin levels in the responder group was significantly different (p=0.044) from the change (-delta) in the prolactin levels in the nonresponder group. Although caution is warranted when interpreting this finding in light of the small number of patients, the phenomenon is intriguing and warrants further research in a larger group of men.
The aforementioned results suggest that in the current group of men with lifelong PE, (1) neither lifelong PE nor the duration of the IELT is associated with serum leptin levels, (2) the serum leptin level is within the range of the normal population, (3) paroxetine treatment-induced ejaculation delay is not associated with serum leptin levels, (4) paroxetine treatment-induced ejaculation delay is not solely related to serum paroxetine levels, (5) paroxetine treatment-induced ejaculation delay is not associated to serum leptin levels, and (6) nonresponse to paroxetine treatment is not related to paroxetine serum levels, serum leptin levels, or the patients' BMI. Instead, it may well be that paroxetine-induced ejaculation delay and nonresponse to paroxetine treatment is associated with 5-HT1A receptor C-1019 G polymorphism or prolactin metabolism or underlying mechanisms of action.
The strengths of the current study were the strict sampling protocol, the measurement of IELT with a stopwatch during a baseline period and during three consecutive 4-week daily paroxetine treatment periods, and the inclusion of SSRI (including paroxetine) nonresponders and paroxetine responders. Another strength was that blood sampling was performed at four different fixed time points in the morning after 12 hours of fasting, at the onset of and after 4 weeks of the baseline period, and after three consecutive daily paroxetine treatment periods with 10-, 20-, and 30-mg paroxetine hemihydrate. Last, serum paroxetine levels and serum leptin, prolactin, and gonadotrophin levels were assessed in relation to the three different dosages of paroxetine, Cyp2D6 assessment, and 5-HT1A receptor polymorphism genotyping. However, a limitation of the current study was the small number of patients.
Although this is the first study investigating SSRI nonresponse in men with lifelong PE, our findings regarding serum leptin levels are not in line with three previous studies on leptin in relation to PE (Table 4). For example, in 2002, Atmaca et al. [9] reported a high serum leptin level of 25.7±3.9 ng/mL in 15 Turkish men with PE compared with 7.9 ±2.1 ng/mL in 15 healthy controls, after adjustment for BMI and age. In a second study, Atmaca et al. [7] reported significantly decreased leptin levels (8.3±2.8 ng/mL) in 15 men with PE after 8 weeks of daily 30.7 ± 9.3 mg citalopram treatment compared with baseline values (23.9±5.3 ng/mL). Atmaca et al. [7] therefore suggested that PE is associated with increased serum leptin levels and that citalopram treatment induces a decrease in leptin. However, although it was mentioned in the latter study that the patients had the same weight at the end of the study, the BMI at the end of the study was not reported. It therefore remains rather unclear whether the decreased leptin level after citalopram treatment was related to a change in the BMI of the PE patients. Notably, in contrast to their first study, the second study of Atmaca et al. [7] reported a high serum leptin concentration in their control males (24.2±3.8 ng/mL). This finding of Atmaca et al. [7] also contrasts the findings of Nikoobakht et al. [10], who in 46 Iranian men with PE found a normal but higher baseline serum leptin level (8.3±3 ng/mL) than in a control group of 44 men with nephrolithiasis (3.3±1 ng/mL).
In our current study, all patients had leptin levels that had a normal value compared to a standard control group. Moreover, our patients, both the responders and the nonresponders, had the same leptin levels, both at baseline and at the end of the three paroxetine treatment periods. Indeed, in our study, both the responders and the nonresponders had an identical BMI at the start and at the end of the study. Thus, there is no reason to believe that lifelong PE or the IELT is related to weight or serum leptin concentrations. Neither is there reason to believe that paroxetine treatment influences or is influenced by serum leptin levels. In other words, on the basis of our study, in which serum leptin and testosterone levels, other gonadotrophic parameters, TSH, T4-free, and BMI remained homogeneous throughout paroxetine treatment in both responders and nonresponders, serum leptin levels cannot be considered a biological marker of PE as has been suggested by Atmaca et al. [7,9] and Nikoobakht et al. [10]. On the contrary, many questions remain regarding leptin that must be investigated in the context of lifelong PE.
As is summarized in Table 5, it is of note that the four studies on leptin, including the current study, used different leptin kits. In the current study, a radioimmunoassay (RIA) method, specific for human leptin, was used, whereas Nikoobakht et al. [10] used an enzyme-linked immune assay method, specific for human leptin. In contrast, Atmaca et al. [7,9] used an RIA method specific for rat leptin to measure human serum leptin concentrations. Although our human kit has a cross-reactivity of 100% with human leptin, the cross-reactivity of the kit used by Atmaca et al. [7,9] is only 40% [15]. However, whether the use of different leptin kits contributed to the different findings of Atmaca et al. [7,9], Nikoobakht et al. [10], and the current study remains unknown.
Another explanation for the different findings may be related to different testosterone levels of the included patients. High testosterone in males has been reported to be associated with low serum leptin levels [8]. Because serum testosterone was not measured in any of the aforementioned studies, it cannot be excluded that the differences between the four studies are related to differences in serum testosterone levels. It is therefore recommended that in future studies on PE and leptin, serum testosterone be measured.
CONCLUSIONS
Using a very strict and elaborate sampling protocol at different daily doses of paroxetine, we found no explanation for the absence of paroxetine-induced ejaculation delay in six men with lifelong PE. Moreover, we found no indication that the level of leptin is associated with the presence of lifelong PE, the dosage or duration of daily paroxetine treatment, the serum level of paroxetine, or the duration of the IELT at baseline or during paroxetine treatment. In addition, we found no evidence that daily use of paroxetine influences plasma leptin levels in either responders or nonresponders to daily paroxetine treatment.
Although it was found that increasing daily doses of paroxetine were associated with a stronger ejaculation delay, we found no association between serum paroxetine concentrations and paroxetine-induced FI of the geometric mean IELT. However, we did find that serum concentrations of paroxetine were higher in two men with the Cyp2D6*3 and *4 variations, respectively. However, because there is no relation between the serum paroxetine concentration and the IELT, this genotype for paroxetine metabolism is not relevant for paroxetine-induced ejaculation delay in the current study. Interestingly, in the current group of men, we found two intriguing phenomenons. First, all paroxetine nonresponders were heterozygous (GC genotype) for the 5-HT1A receptor C-1019G variation, whereas all responders had the wildtype (CC) genotype. However, although we have argued that these results may be related to a selection bias, further research in a larger group of men with lifelong PE is warranted to investigate whether this polymorphism plays a role in paroxetine treatment nonresponse. Second, serum prolactin levels increased in the paroxetine responders, whereas they tended to decrease in the paroxetine nonresponders. The change in prolactin serum level after paroxetine treatment in the responders was significantly different compared with the prolactin serum level change in the nonresponders. This phenomenon deserves further investigation in future studies.







 XML Download
XML Download