

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Urinary tract infection (UTI) is a common disease in children [1]. The prevalence of UTI in males and females is 2% and 7%-8%, respectively [2]. UTI includes acute pyelonephritis, lower UTI, and asymptomatic bacteriuria. Acute pyelonephritis is the most severe type of the disease [1,2,3]. Serious complications, such as renal scarring, hypertension, and chronic renal failure can result following a delay in diagnosis and treatment. In addition, failure to detect risk factors may aggravate complications [4,5,6,7]. The prevalence of renal scarring following febrile UTI has been reported as 10% to 65% [8]. Risk factors, including sex, not being circumcised, constipation, and vesicoureteral reflux (VUR), increase the incidence of UTI [2,9]. VUR is the most important risk factor for UTI. VUR is the backflow of urine from the bladder to the ureter and, in some cases, to the pelvis and calyces [10]. Previous studies suggest that the prevalence of VUR in children ranges from 25% to 40% [10,11].
Although voiding cystourethrography (VCUG) is currently used as a reliable imaging method for diagnosing VUR, it is painful and expensive and exposes the patient to radiation. Furthermore, iatrogenic UTI may appear after catheterization [10,12]. Considering the side effects of VCUG, the lack of VUR in more than 50% of children with UTI, and the spontaneous recovery from low-grade VUR, researchers have sought cost-effective noninvasive markers for predicting VUR [13,14,15]. Soylu et al. [16] reported that fever higher than 38℃ and C-reactive protein (CRP) of more than 50 mg/dL were suitable predictive markers for the presence of VUR and high-grade VUR, respectively. In this regard, the present study was conducted to determine the predictive value of clinical, laboratory, and imaging findings in the diagnosis of VUR in children with their first febrile UTI.
MATERIALS AND METHODS
This prospective cross-sectional study examined 153 children aged 1 month to 12 years with their first diagnosed febrile UTI in Qazvin's Children's Hospital, Qazvin, Iran, in 2012 through 2013. This hospital is the only referral hospital for children in Qazvin province that is affiliated with the Qazvin University of Medical Sciences. The sample size was calculated on the basis of P=58% (sensitivity for feve r>38.5℃ to discriminate patients to correct groups), d=0.08, α=0.05, 1-α=0.95, β=0.2, and 1-β (statistical power of study)=0.8 [16] and by using the following equation:  Consecutive sampling continued until the desired sample size was reached.
Consecutive sampling continued until the desired sample size was reached.
Consecutive sampling continued until the desired sample size was reached.The inclusion criteria for children with febrile UTI were as follows: (1) first febrile UTI; (2) having symptoms of febrile UTI, such as fever, chills, vomiting, diarrhea, and irritability in infants, and fever, vomiting, abdominal and flank pain, dysuria, and frequency in children; (3) abnormal urinalysis (the presence of leukocyturia, a positive urinary nitrite test, etc.); (4) positive urine culture (urine culture more than 1×105 colonies of a single pathogen in a midstream urine sample or clean catch method or 1×104 colonies of a single pathogen via urinary catheterization, or presence of any number of colonies of organism in urine culture taken by suprapubic method) [3,10]; (5) performance of renal ultrasound, dimercaptosuccinic acid (DMSA) renal scanning, and VCUG. Children meeting the following criteria were excluded from the study: (1) using antibiotics; (2) failing to undergo VCUG; (3) having accompanying and underlying disease, such as septicemia and immune disorders; and (4) having structural abnormalities of the urinary system (such as ureteropelvic junction obstruction, neurogenic bladder, etc.) except VUR.
First, the symptoms of the disease were recorded, and, before the start of antibiotic therapy, serum samples were delivered to the laboratory to test white blood cell count, neutrophil count, platelet count, erythrocyte sedimentation rate (ESR), and CRP quantitative level. All laboratory examinations were performed by use of standard methods in the laboratory department of Qazvin Children Hospital. The renal ultrasound was performed within the first 48 hours of admission, the renal VCUG was performed at the end of treatment when the patients were discharged from the hospital, and the DMSA renal scan was done in the first week of admission [3,10]. The ultrasound and VCUG were carried out by a radiologist, and the DMSA renal scan was performed and interpreted by a nuclear medicine specialist. All patients were studied under similar conditions.
Any report of hydronephrosis or hydroureteronephrosis without evidence of mechanical obstructions, such as ureteropelvic junction obstruction, ureterovesical Junction obstruction, and posterior urethral valves, in the renal ultrasound, and any report of reduced uptake on the DMSA renal scan for pyelonephritic changes in the kidneys were considered as suspicious for VUR [3]. According to the results of the VCUG, the patients were divided into two groups: a group with VUR and a group without VUR. The severity of VUR was graded according to the International Study of Reflux in children [17]. Grades 1 and 2 were regarded as low-grade VUR, and grades 3, 4, and 5 were regarded as high-grade VUR [16].
The sensitivity, specificity, positive (PPV) and negative predictive value (NPV), positive (LRP) and negative likelihood ratio (LRN), and accuracy of the clinical, laboratory, and imaging variables for diagnosis of VUR were determined. Chi-square test, exact test, t-test, and nonparametric tests (Mann-Whitney test) were applied to analyze the obtained data. All analyses were performed with SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). A p-value less than 0.05 was considered statistically significant.
All parents were provided information regarding the research method in simple language. The children were included in the study after their parents agreed and signed the informed consent form.
RESULTS
Of the 153 studied patients, the male-to-female ratio was 18:135. The median±interquartile range of the patients' ages was 29±49 months. The most frequent symptoms in decreasing frequency were fever (100%), chills (62.7%), and dysuria (42.5%). The most frequently grown microorganism in the urine culture was Escherichia coli (80.3%). Of the 153 studied patients, VUR was observed in 60 (39.2%).
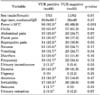
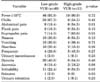
Comparisons of the different variables between children with and without VUR and also between the low-grade and high-grade VUR groups are shown in Tables 1, 2, 3, 4. By use of receiver operating characteristic curve analysis, it was shown that for predicting VUR in children with febrile UTI, CRP≥20 mg/dL had a sensitivity of 61% (95% confidence limit [CL], 49-74), specificity of 57% (95% CL, 46-67), LRP of 1.43, and accuracy of 58%. In addition, fever≥38.2℃ had a sensitivity of 60% (95% CL, 47-72), specificity of 53% (95% CL, 42-62), LRP of 1.26, and accuracy of 55.5% (Table 5).
The sensitivity, specificity, LRP, and accuracy of the DMSA renal scan for predicting VUR were 63% (95% CL, 51-75), 96% (95% CL, 91-99), 14.7, and 79.5%, respectively. Also, those of the renal ultrasound were 30% (95% CL, 18-41), 96% (95% CL, 85-97), 3.4, and 60.5%, respectively. The multivariate logistic regression analysis revealed significant positive correlations between fever>38.2℃ and DMSA renal scan and VUR, and also between ESR, positive urinary nitrite test, hyaline cast, and ultrasound and high-grade VUR (Table 6).
DISCUSSION
This study showed that the best predictive markers for the presence of VUR in children with their first febrile UTI are fever>38.2℃ and DMSA renal scan. In addition, for high-grade VUR, ESR, positive urinary nitrite test, hyaline cast, and ultrasound were the best predictive markers. Many researchers and resources recommend that all children with their first UTI undergo VCUG [18,19,20,21]. Given than only 25% to 40% of children with UTI have VUR and that VCUG is invasive and expensive and exposes the gonads to radiation [10,12], researchers have looked for noninvasive markers for predicting VUR to avoid unnecessary VCUG.
For example, Soylu et al. [16]'s study on 88 children with febrile UTI revealed a significant difference between two groups with and without VUR in terms of fever≥38.5℃, pyuria≥25/high power field, and CRP≥23.5 mg/L. However, logistic regression analyses showed that only fever≥38.5℃ was an appropriate predictor of the presence of VUR. Moreover, the above researchers revealed that CRP≥50 mg/dL was a suitable predictor for the presence of high-grade VUR [16]. Oostenbrink et al. [22] performed a study on 140 children less than 5 years old with their first febrile UTI and assessed variables including age, sex, and family history of UTI, CRP, and renal ultrasound. Their clinical approach yielded a sensitivity of 100% and specificity of 17% for predicting all VUR grades and a sensitivity of 100% and specificity of 38% for predicting VUR grade≥III. A similar study conducted by Leroy et al. [23] on 149 children aged 1 month to 4 years with their first febrile UTI did not confirm the results of Oostenbrink's study.
The results of the present study were somewhat similar to those of the studies by Soylu et al. [16] and Oostenbrink et al. [22]. Although the quantitative CRP level, RBC count in urine, results of renal ultrasound, and DMSA renal scan showed a significant difference between the groups with and without VUR in the present study, the multivariate logistic regression analysis revealed a significant positive correlation between fever>38.2℃ and renal DMSA scan and VUR. Also, although there was a significant difference between the low-grade VUR and high-grade VUR groups regarding the neutrophil count, ESR, leukocyturia, positive urinary nitrite, and ultrasound results, the multivariate logistic regression showed a significant positive correlation of high-grade VUR with ESR, positive urinary nitrite test, hyaline cast, and renal ultrasound.
In a study by Tseng et al. [24] on 142 children less than 2 years old with their first febrile UTI, the authors reported that the sensitivity, specificity, positive predictive value, and negative predictive value of DMSA renal scan in predicting VUR were 88%, 37%, 36%, and 88%, respectively. The above authors concluded that children with a normal DMSA renal scan rarely had VUR and never had high-grade VUR [24]. A study conducted by Camacho et al. [25] on 152 children with their first febrile UTI showed that VUR was more frequent in children with an abnormal DMSA renal scan than in children with a normal DMSA renal scan (48% vs. 12%). The above researchers concluded that the risk of renal damage was very low in children with their first febrile UTI and a normal DMSA renal scan.
Another study pointed out the predictive value of DMSA renal scan and renal ultrasound in the diagnosis of high-grade VUR. That study reported the detection rate of ultrasound for low- and high-grade VUR to be 86% and 41.7%, respectively, and that of the DMSA renal scan for low- and high-grade VUR to be 88.4% and 37.5%, respectively [26]. On the contrary, Sorkhi et al. [27] reported that the DMSA renal scan alone or along with renal ultrasound could not predict VUR. Therefore, they argued that VCUG must be done to diagnose VUR.
In the present study, the highest LRP was respectively related to the DMSA renal scan, renal ultrasound, CRP≥20 mg/dL, and fever higher than 38.2℃. The DMSA scan had high sensitivity and specificity for the diagnosis of VUR. In this respect, similar to the studies of Tseng et al. [24] and Camacho et al. [25], it can be concluded that in the case of a normal DMSA scan, the risk of VUR is very low, and performing VCUG is unnecessary. Although some studies mentioned procalcitonin as a predictor of VUR, the relevant test is more costly than other routine tests, such as CRP and ESR, and is not available everywhere [28]. We hope that the results of the present study will help to avoid unnecessary VCUG in children affected by their first febrile UTI. Given that the present study was conducted in one educational hospital, further multicenter studies are recommended.
CONCLUSIONS
This study revealed that the best predictive markers for the presence of VUR in children with their first febrile UTI are the fever>38.2℃ and DMSA renal scan. ESR, positive urinary nitrite test, hyaline cast, and renal ultrasound are best predictive markers for the presence of high-grade VUR.




 XML Download
XML Download