

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Vesicoenteric fistula is a rare disease, with an estimated 2 to 3 patients per 10,000 hospital admissions and with an annual incidence of 0.5 per 100,000 [1]. Vesicoenteric fistula is usually secondary to an inflammatory or malignant bowel etiology such as diverticulitis, colorectal carcinoma, or Crohn's disease [2]. Vesicoenteric fistula due to primary bladder squamous cell carcinoma is extremely rare. Here we report the case of patient with a vesicoenteric fistula secondary to bladder squamous cell carcinoma.
CASE REPORT
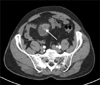
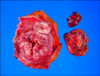
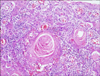
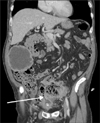
A 70-year-old male patient presented with painless, total gross hematuria. He had a history of urethral stricture due to a motor vehicle accident, and visual internal urethrotomy had been performed 9 years previously. He also had hypertension that was being treated medically. Abdominopelvic computed tomography (CT) showed an approximately 2.7-cm lobulated and contoured enhancing mass in the bladder dome within the diverticulum with no definite pelvic lymph node enlargement (Fig. 1). After transurethral resection of the bladder tumor, we performed a partial cystectomy at the bladder dome. Because the tumor was a small 2.7-cm mass, without pelvic lymph node enlargement, and limited to the bladder dome on CT, we performed partial cystectomy. The margins were negative in the frozen biopsy. Grossly, firm whitish gray masses were seen (Fig. 2). The pathology report was squamous cell carcinoma, infiltrating the serosa. Microscopically, the bladder tumor was composed of keratin-producing malignant cells (Fig. 3).
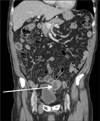
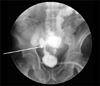
Three months postoperatively, frequency and nocturia occurred. Follow-up abdominopelvic CT showed a new approximately 4.7-cm×4.0-cm lobulate, heterogeneous mass in the dome of the bladder. CT also revealed another 2.9-cm×2.3-cm hypodense mass with peripheral rim enhancement in the right upper abdomen (Fig. 4). After we inserted a Foley catheter, bowel materials and feces were evacuated through the Foley catheter. Cystography showed that contrast media leaked to the ileum (Fig. 5). Abdominopelvic CT showed an enlarged mass at the dome of the bladder and noted communication with the sigmoid colon (Fig. 6). Ileostomy was done in the department of surgery. Eventually, bladder squamous cell carcinoma spread to multiple organs and the patient died of multiple organ failure 6 months later.
DISCUSSION
Vesicoenteric fistulas are usually secondary to an inflammation or malignancy of the bowel such as diverticulitis (52%), Crohn's disease (18%), carcinoma of the colon (11%), or other malignant pelvic conditions (9%) and uncommonly to infection, trauma, radiation, or iatrogenic surgical trauma [2]. Few cases of urological vesicoenteric fistulas have been described in the literature, and most of these were in the form of isolated case reports [3]. The peak incidence of vesicoenteric fistula is between 55 and 65 years of age.
The most common clinical presentations of vesicoenteric fistulas are urinary tract infection (100%), pneumaturia (66%), fecaluria (50%), and hematuria (22.6%) [4], because the high bladder compliance and low intravesical pressure favor the unidirectional flow of bowel contents to the bladder. The classical presentation of vesicoenteric fistula is described as Gouverneur's syndrome and consists of suprapubic pain, urinary frequency, dysuria, and tenesmus [5]. Thus, in some case, if refractory to antibiotic therapy, urinary tract infection may suggest a vesicoenteric fistula. Vesicoenteric fistula can be diagnosed by use of tests such as cystoscopic examination, cystography, excretory urography, barium enema, and CT. Cystoscopic examination is the most sensitive investigation, with accuracy of 79% [6]. Sometimes, nonspecific and localized erythema and a papillary lesion make diagnosis difficult. Cystography, excretory urography, and barium enema with or without the small bowel have lower detection rates of 20% to 35% [6]. Cross-sectional imaging, especially CT scanning, has become the imaging modality of choice [5]. In CT findings, bladder wall thickening adjacent to the loop of thickened colon, bladder air, and colonic diverticula are suspicious of vesicoenteric fistula. Oral ingestion of activated charcoal will appear in the urine as black particles in cases of vesicoenteric fistulas [5]. Our case revealed bladder wall thickening adjacent to the loop of thickened bowel and bladder air in the CT.
Both single and multistage procedures have been advocated in the treatment of vesicoenteric fistulas, depending on the clinical circumstances. Some medical treatments, such as octreotide, are also available for malignant vesicoenteric fistula [7]. In surgical treatment, minimally invasive and organ-preserving surgery, such as laparoscopic bladder-preserving surgery, should be performed in the case of a vesicoenteric fistula caused by benign diseases [8]. In a malignant vesicoenteric fistula, Whiteley Jr and Grabstald [9] proposed that a one-stage en bloc resection of the colonic malignancy and involved bladder portion is a reasonable and safe procedure, thus avoiding a total cystectomy [3,4]. Vidal Sans et al. [10], however, reported that surgical morbidity and mortality is relatively high, especially in fistula resulting from malignancy.
 XML Download
XML Download