

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ureteral stent placement is frequently performed for the relief of benign or malignant obstructions, perioperatively as an adjunct to stone therapy, and in the management of urinary leakage. Complications related to ureteral stent indwelling are not uncommon because the technique is used so frequently, but most are mild. Other complications involving adjacent vascular structures are rare, and the most common is arterio-ureteral fistula. Without prompt and appropriate management, such complications can be fatal. They can arise in several situations, including in extirpative surgery for malignant pelvic or abdominal disease, with previous vascular reconstruction procedures, and in degenerative iliac artery disease [1,2]. Vein complications involving the ureter are even less common than are arterial complications. We report an extremely rare case of cardiac migration of a ureteral double J (D-J) stent after a ureteroneocystostomy.
CASE REPORT
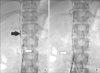
A 29-year-old woman visited Pusan National University Hospital with mild back pain when coughing and suprapubic discomfort after voiding. According to her medical history, she had undergone a hysterectomy 2 weeks earlier for uterine atony during a caesarean section and right-sided ureteroneocystostomy with bladder rupture repair after a right lower ureteral transaction injury. A ureteral D-J stent (6 Fr, 26 cm) was placed intraoperatively in the right urinary tract to prevent urinary leakage. No intra- or postoperative radiological evaluation was performed. Intravenous pyelography (IVP) on day 2 after admission showed that the D-J stent extruded from the urinary tract (Fig. 1A). We could not find the distal end of the ureteral stent during a cystoscopic evaluation and considered removing the stent laparoscopically. Preoperative laboratory findings, including urine analysis, were normal except for a slight increase in C-reactive protein levels (0.75 mg/dL). Abdominopelvic computed tomography (CT) on day 3 after admission revealed that the ureteral stent had migrated further upward into the right cardiac chamber (Fig. 1B, C). We changed our treatment plan and decided on endovascular management to reduce the possibility of any morbidity or mortality related to open surgery.
Before the radiological intervention, a scout x-ray examination showed that the distal end of the stent had migrated to the L1 vertebral level. The percutaneous approach was transfemoral on both sides and a 9-Fr sheath and 5-Fr sheath were indwelled in the right and left common femoral veins, respectively. A pigtail catheter extending from the left femoral sheath separated the distal end of the ureteral D-J stent from the right ovarian vein, and a snare loop from the right femoral sheath then drew the stent from the vascular circulation (Fig. 2A, B). Inferior venography after the procedure showed no fistula tract or bleeding focus. The patient was discharged on day 5 after admission, and her postoperative course was uneventful. The follow-up CT and IVP showed normal urinary and vascular structures 5 months later.
DISCUSSION
Double pigtail ureteral stents are flexible and are designed to curl at both ends, which prevents ureteral injury and stent migration. However, ureteral stents are so frequently indwelled that consequences or complications are not uncommon. An interventional procedure or open surgery is required when a ureteral stent penetrates the ureteral wall or migrates outside the urinary tract [3,4].
There are two possible mechanisms or etiologies in the present case. The first is the simultaneous perforation of the lower ureteral wall and one of the adjacent intercommunicating ovarian veins during the retrograde placement of the ureteral D-J stent. The mechanism underlying the complication probably involved the proximal migration of the stent, with the withdrawal of its distal curl within the distal third of the ureter, causing the simultaneous perforation of the ureteral wall and one of the adjacent intercommunicating ovarian veins [5]. Ioannou et al. [6] and Falahatkar et al. [7] reported that a ureteral pigtail stent that was placed retrogradely in a patient with obstructive nephropathy migrated into the inferior vena cava after simultaneous perforation of the ureter and iliac vein. The second possible etiology involves the misplacement of the ureteral D-J stent into the transected ovarian vein, which had been mistaken for the ureteral end. Our patient underwent a hysterectomy for uterine atony, and massive hemorrhage and bladder rupture occurred during the hysterectomy and hemostasis. We suggest that in that urgent and deleterious surgical situation, the surgeon mistook the transected ovarian vein for the ureter and anastomosed the right ovarian vein to the bladder. Under those specific conditions, the ureteral D-J stent may have been indwelled via the anastomosed ovarian vein, flowing into the inferior vena cava.
The management of a ureteral stent that has migrated into the vascular circulation includes open surgical techniques, interventional radiological techniques, and combinations of both [8]. Kidd 3rd et al. [3] reported the open surgical removal of a migrated pigtail ureteral stent in a patient with ureteral and renal vein perforation and placement of the stent into the renal vein. Ioannou et al. [6] reported that a pigtail ureteral stent that had migrated into the inferior vena cava was removed through a lateral incision in the anterior surface of the left common iliac vein. Michalopoulos et al. [5] removed a pigtail ureteral stent that had migrated into the left pulmonary artery with an endovascular procedure, which was performed through the right femoral vein. In the present case, an endovascular procedure was selected for removing the migrated ureteral D-J stent for several reasons. First, the patient's vital signs were stable and there was no retroperitoneal hemorrhage or active bleeding focus on abdominal CT. Second, the ureteral stent had migrated completely from the urinary tract to the vascular circulation. Third, there was no need to replace the ureteral stent because the injured urinary tract was intact and no contrast leakage was seen on IVP or CT. Fourth, this procedure was performed to minimize the risk of morbidity that follows open heart or vascular surgery.
Several factors should be considered to prevent the intraoperative misplacement or malposition of a ureteral stent. The reflux of a methylene blue irrigant from the bladder can be observed to verify the appropriate placement of the stent after ureteroneocystostomy [9]. Ureteral stents can be placed safely with fluoroscopic assistance, and any positioning problems can be identified and corrected at the time of insertion [10]. After insertion, the anatomical position of the stent can be estimated on an anteroposterior abdominal radiograph [5]. In our patient, the ureteral stent was placed without fluoroscopic assistance and no radiological examination was performed during or after the operation. In conclusion, extensive pelvic surgery with massive hemorrhage is frequently accompanied by urinary tract injury. When a ureteral stent is indwelled, it is mandatory to evaluate whether the stent has been inserted anatomically appropriately. When a ureteral stent migrates completely from the urinary tract to the vascular circulation, an endovascular procedure is a good treatment option.

 XML Download
XML Download