

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Despite the increased incidence of prostate cancer over the past two decades, patient survival has improved because the widespread use of serum prostate-specific antigen (PSA) as a diagnostic marker has enabled prostate cancer to be diagnosed at an early stage [1,2]. As a result of increased surveillance, physician awareness of patients developing other primary malignancies during long-term follow-up has also increased [3]. Multiple primary malignancies develop in about 5% to 16% of all cancer patients, which is 20% to 31% higher than the expected cancer occurrence in the general population [3,4]. Furthermore, the genitourinary system is a frequently involved region of multiple primary malignancies [5,6].
We are concerned about the effect of other primary malignancies on survival in prostate cancer patients. Although several studies have investigated the prevalence and the prognosis of multiple primary malignancies in other cancers [7,8,9,10], no consensus about prognosis exists and information about the association of prostate cancer with other primary malignancies is limited [11,12,13]. Therefore, studying the potential association of prostate cancer with other primary malignancies is critical to developing guidelines for treatment modalities and to effectively predict the prognosis of prostate cancer.
We investigated clinicopathological characteristics, biochemical recurrence (BCR)-free survival, overall survival (OS), and prostate cancer-specific survival (CSS) in prostate cancer patients with or without other primary malignancies who had undergone radical prostatectomy (RP).
MATERIALS AND METHODS
1. Patient population and pathological assessment
After obtaining institutional review board approval, we retrospectively reviewed the medical records of 1,070 patients who underwent open RP and of 247 patients who underwent robot-assisted laparoscopic prostatectomy for prostate cancer at our institution between 1990 and 2008. All patients underwent pelvic lymphadenectomy. These surgeries were performed by three surgeons. Patients with prior hormonal therapy or radiation therapy were excluded from the study, as were patients with missing follow-up data. The presence of other primary malignancies was entered into the database prospectively, and we reviewed the patients' medical records retrospectively.
All patients underwent preoperative evaluation, including a clinical examination, blood tests, a chest x-ray, magnetic resonance imaging, and bone scanning. We assessed the patients' age at the time of surgery, preoperative PSA concentration, biopsy Gleason score (GS), clinical stage, pathological GS, pathological stage, surgical margin status, and lymph node status. RP specimens were examined microscopically after histological sectioning at multiple levels after formaldehyde fixation. Surgical margins were considered positive if tumor cells were touching the ink on the specimen surface [14]. Pathological staging was determined by using the sixth edition of the American Joint Committee on Cancer TNM staging [15]. Tumor differentiation was evaluated by surgical Gleason scoring according to consensus conference recommendations of the World Health Organization [16].
All patients were followed up every 3 months for the first year, semiannually during the second year, and annually thereafter. Each visit included a clinical examination and PSA measurement. BCR was defined as any increase in PSA concentration to ≥0.2 ng/mL and a second confirmatory value [17]. Cause of death was attributed to prostate cancer if prostate cancer was recorded as the underlying cause of death or if a patient with hormone-refractory metastatic prostate cancer died.
2. Cancer classification
The Warren and Gates criteria were used to diagnose other primary cancers: (1) the cancer must be clearly malignant as determined by histologic evaluation, (2) each cancer must be geographically separate and distinct, and (3) the possibility that the second cancer represents metastasis should be eliminated [18]. All pathological prostate cancer specimens were confirmed to be adenocarcinoma that had not metastasized from other primary malignancies. Prostate cancer patients with other primary malignancies were subdivided into two groups according to the time of other primary malignancy diagnosis. Patients who had other primary malignancies diagnosed previously or concomitantly when we detected prostate cancer were assigned to group 1, and patients who were only diagnosed with other primary malignancies after RP for prostate cancer were assigned to group 2.
3. Statistical analysis
Clinicopathological factors were compared between the two groups by using Student t-test or a Mann-Whitney U test for continuous variables and Pearson chi-square test or Fisher exact test for categorical variables. BCR-free survival, OS, and CSS were analyzed by using the Kaplan-Meier method and were compared by using the log-rank test. A Cox proportional hazards regression model was used to estimate the prognostic significance of each variable. Correlations between the assessed variables and BCR-free survival, OS, and CSS were expressed as hazard ratios with 95% confidence intevals. All statistical tests were two-tailed, and p<0.05 was considered significant. The SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
RESULTS
At least one additional primary malignancy was detected in 187 of the 1,317 prostate cancer patients (14.2%). In particular, 178 patients were affected by one other primary malignancy and 9 patients by two other primary malignancies for a total of 196 prostate cancer-associated other primary malignancies. The most common site of other primary malignancies was the colorectum (23.0%) (Table 1).
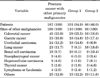
Clinicopathological features according to the presence or absence of other primary malignancies and the time to other primary malignancy diagnosis are shown in Table 2. No significant differences in clinical and pathological variables were observed between prostate cancer patients with other primary malignancies and those without other primary malignancies, except for patient age. Prostate cancer patients with other primary malignancies were older than patients without other primary malignancies (p<0.001). No significant differences in clinical and pathological variables were found according to the time to other primary malignancy diagnosis, except for the pathological GS. Group 2 had a higher proportion of pathological GS ≥8 than did group 1 (p=0.048).
At a mean follow-up time of 49.6 months, 263 patients (20.0%) had a BCR, and 141 patients (10.7%) died (25 from prostate cancer). A comparison of BCR-free survival between prostate cancer patients with and those without other primary malignancies is shown in Fig. 1A. No significant differences (p=0.656) in BCR-free survival were found between these two patient groups, respectively: 5-year BCR-free survival (80.2% compared with 77.7%) and 10-year BCR-free survival (67.3% compared with 70.4%). A comparison of BCR-free survival between the three groups, according to the time when other primary malignancies were diagnosed, is shown in Fig. 1B. No differences (p=0.146) in BCR-free survival were found between those without other primary malignancies, those in group 1, and those in group 2, respectively: 5-year BCR-free survival (80.2%, 87.6%, and 67.0%) and 10-year BCR-free survival (67.3%, 80.2%, and 60.3%). However, when we compared BCR-free survival between only group 1 and group 2, survival was significantly lower in group 2 (p=0.003).
Significant differences (p<0.001) in OS between prostate cancer patients with and without other primary malignancies, respectively, are shown in Fig. 1C: 5-year OS (95.4% and 89.3%) and 10-year BCR-free survival (84.5% and 62.5%). Furthermore, a significant difference (p<0.001) in OS was found according to the time of diagnosis of other primary malignancies: 5-year OS (95.4%, 83.1%, and 83.1%) and 10-year OS (184.5%, 82.6%, and 44.6%) (Fig. 1D). On the other hand, as shown in Fig. 1E, no significant differences (p=0.733) in CSS were found between prostate cancer patients without other primary malignancies and patients with other primary malignancies, respectively: 5-year CSS (98.9% compared with 98.5%) and 10-year CSS (96.8% compared with 96.3%). Moreover, no significant difference (p=0.755) in CSS was found according to the time of other primary malignancy diagnosis: 5-year CSS (99.0%, 99.0%, and 98.2%) and 10-year CSS (97.2%, 99.0%, and 93.0%) (Fig. 1F).
Multivariate Cox regression analyses of variables predicting BCR showed that pathological GS, pathological stage, and positive surgical margin were independent predictors of BCR. The presence of other primary malignancies did not independently predict BCR. On multivariate Cox regression analyses of variables predicting OS, other primary malignancies diagnosed after RP for prostate cancer, age at surgery, pathological GS, lymph node metastasis, and positive surgical margin were independent predictors of OS (Table 3). Conversely, pathological stage and lymph node metastasis were the only independent predictors of CSS. Other primary malignancies diagnosed before RP for prostate cancer did not affect OS or CSS.
DISCUSSION
Because of increased longevity and a parallel increase in survival after cancer-specific treatment, the number of multiple primary malignancies has continued to increase [3]. Although the etiology of multiple primary cancers is complex, the frequent occurrence of multiple primary malignancies may be due to increased detection rates. The routine use of more accurate diagnostic and imaging modalities during staging and preoperative work-ups and intensive follow-up of patients with one primary cancer contribute to increased detection. Additionally, the prolonged survival of cancer patients as a result of improved treatment modalities, exposure to environmental carcinogens, unhealthy habits and lifestyles (e.g., smoking, obesity), and an impaired immune system may increase the onset or the detection of other primary cancers [19,20,21]. Taken together, these factors increase the chance of diagnosing other primary malignancies in a prostate cancer patient.
In previous studies, the frequency of other primary malignancies in prostate cancer was 9%-12.5%, and the most common sites of other primary malignancies were the colorectum, lung, kidney, and bladder [3,8]. These results are similar to data from previous studies, except for the higher incidence of gastric cancer that we detected.
Despite the increased incidence of colorectal cancer, patient survival has improved [22,23]. The detection rate of colorectal cancers in patients with prostate cancer increased; however, increased detection vigilance alone cannot fully explain the correlation between colorectal cancer and prostate cancer. Another explanation is Asian societal changes to a more Western lifestyle, including a higher dietary fat content [24]. Dietary fat intake and obesity have been independently associated with increased prostate and colon cancer rates [25].
A higher incidence of gastric cancer was observed in our study than in most previous studies [3,8]. However, a Japanese study reported the most common site of other primary malignancies was the stomach [13]. Furthermore, gastric cancer is the most frequently occurring cancer in East Asian countries, unlike in western countries [22]. Therefore, the higher incidence of gastric cancer in our study might be explained by differences in the prevalence of this specific cancer between Asian and western countries.
Prostate cancer patients with other primary cancers were older than those without other primary malignancies. However, other clinicopathological features were not significantly different between the two groups in our study. A previous study reported that the prostate cancer stage was lower in patients with other primary malignancies than in patients without other primary malignancies because of early detection of the second primary malignancy [13]. In that study, however, other primary malignancies were diagnosed before prostate cancer in most patients. Our study included similar patient numbers in the groups in which other primary malignancies were diagnosed either before or after prostate cancer detection. Thus, we observed that prostate cancer associated with other primary malignancies did not show more advanced staging than prostate cancer without other primary malignancies. These results confirm that aging itself is a risk factor for cancer onset. The mechanisms relating cancer and aging include the following: (1) duration of carcinogenesis (the longer a person lives, the more likely it is that carcinogenesis will be completed and cancer will develop), (2) molecular changes with age (older tissues are susceptible to environmental carcinogenesis and undergo molecular changes similar to carcinogenesis), and (3) changes in the environment (aging is associated with molecular changes in DNA signaling and the body environment that may favor the development of cancer) [26].
BCR-free survival rates were not significantly affected by the presence of other primary malignancies in prostate cancer patients. However, comparison of two groups according to the date of diagnosis of other primary cancers showed that BCR-free survival was significantly lower in patients with other primary malignancies diagnosed after, rather than before, RP for prostate cancer. This probably resulted because the pathological GS of prostate cancer was of a significantly higher grade in patients with other primary malignancies diagnosed after, rather than before, RP. This may have been due to a detection bias from the staging investigations and a surveillance bias during evaluation for other primary cancers. Perhaps in patients with a diagnosis of other primary malignancies previously or concomitantly when we detected prostate cancer, the intensive medical follow-up after index cancer detection may have allowed for early detection of the prostate cancer and improved BCR-free survival. In addition, when BCR occurred in prostate cancer patients, we evaluated patients by bone scan and computed tomography to determine whether it represented a locally persistent disease or systemic disease. Therefore, it is possible to increase the incidence of other primary malignancies in BCR patients using detailed imaging. However, after multivariate analysis, the presence of other primary malignancies was not an independent predictor of BCR. These data show that the association between prostate cancer and other primary malignancies is not a negative prognostic factor for BCR.
The current study showed that the association between prostate cancer and other primary malignancies does not constitute a negative prognostic factor for prostate CSS. However, OS was significantly lower in prostate cancer patients with additional malignancies. This was probably a consequence of deaths due to the progression of the other primary malignancies, of the morbidity induced by antitumor treatments, and of the higher age and age-related comorbidities. Matzkin and Braf [21] found that when two different organs or systems are involved by different cancers, the prognosis depends on the second primary malignancy. In agreement with previous studies [13,21], other primary malignancies diagnosed after RP for prostate cancer especially decreased overall patient survival, and other primary malignancies were the major cause of death in the current study. On the other hand, other primary malignancies diagnosed before RP for prostate cancer did not affect prostate cancer prognosis. In light of these facts, a previous history of other primary cancers should not contraindicate the definitive treatment of prostate cancer, especially of organ-confined tumors, which was the case in the large majority of our patients. Because the prognosis for patients with multiple primary malignancies may be improved by both early detection of the second primary malignancy via thorough examination and suitable treatment during follow-up of the index cancer, screening for other primary malignancies is important in prostate cancer patients.
Our study had several limitations. First, this study was retrospective in design and had an inherent selection bias. We analyzed only patients who underwent RP at our institution, excluding patients who received neoadjuvant androgen-deprivation therapy or radiation therapy. Thus, the incidence of prostate cancer-associated other primary malignancies seemed to be underestimated. Furthermore, other primary malignancies diagnosed before RP for prostate cancer may be almost no evidence of disease status, and this selection bias could affect OS. Second, the prevalence of specific types of cancer differs between Asian and western populations. For example, the incidence of gastric cancer is very high in East Asian countries, but not in western countries. Thus, the frequent sites of other primary malignancies could differ between countries and ethnic populations. Nevertheless, we believe that this study was the first to analyze clinicopathological features and factors that predict BCR-free survival, OS, and CSS in prostate cancer patients associated with other primary malignancies who underwent RP.
CONCLUSIONS
In patients who underwent RP for prostate cancer, we observed a 14.2% incidence of other primary malignancies, and the most common site was the colorectum. We conclude that the presence of other primary malignancies is frequent in prostate cancer patients, and this frequency increases with patient age. Furthermore, prostate cancer prognosis after RP is not dependent on the presence of other primary malignancies. However, other primary malignancies diagnosed after RP for prostate cancer had a negative effect on overall patient survival.



 XML Download
XML Download