

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital adrenal hyperplasia (CAH) is an autosomal recessive adrenal steroid synthesis disorder that is transferred genetically and is characterized by increased adrenocorticotropic hormone (ACTH) secretion due to glucocorticoid and mineralocorticoid deficiency [1]. An increase in ACTH synthesis can result in hyperplasia of ACTH-sensitive tissues in the adrenal glands and other sites such as the testes, leading to testicular masses widely known as TART, or testicular adrenal rest tumor [2].
TART is often an asymptomatic benign lesion that frequently occurs in male CAH patients with a reported prevalence of up to 94% [3]. Yet, the prevalence, etiology, and functional features of testicular tumors due to 11β-hydroxylase deficiency are not clearly known. The present article is a case study of bilateral TART in a patient with 11β-hydroxylase deficiency-driven CAH.
CASE REPORT
A 16-year-old male patient was referred from the pediatrics clinic to our clinic with a diagnosis of 11β-hydroxylase deficiency-driven CAH after the determination of bilateral testicular masses. The patient's history revealed a diagnosis of 11β-hydroxylase deficiency-driven CAH at a young age. Although the patient's laboratory data from an early age were not available, the patient had been using dexamethasone 1×0.75 mg and spironolactone 1×100 mg irregularly.
The physical examination revealed multiple bilateral solid nodules in the testes of approximately 0.5 to 1.5 cm. The results of routine hematologic and biochemical tests and the levels of prolactin, luteinizing hormone, and follicle-stimulating hormone were normal. The testosterone level was at the lower limit (231.6 ng/dL). The values of serum markers for testis tumors, such as alpha-fetoprotein (AFP), beta-human chorionic gonadotropin (βhCG), and lactate dehydrogenase (LDH), were within normal ranges. Cortisol, ACTH, and dehydroepiandrosterone sulfate levels were likewise normal, unlike the elevated levels of 17-hydroxyprogesterone and 11-deoxycortisol, which were 23 ng/mL (<2 ng/mL) and 238 ng/mL (<8 ng/mL), respectively.
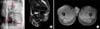
Scrotal ultrasonography revealed the following testicular sizes: right, 41 mm×21 mm, and left, 43 mm×22 mm. Both testes contained multiple solid heterogenic hypoechoic nodules of different sizes ranging from approximately 21 mm×15 mm to 14 mm×10 mm with well-drawn borders and increased vascularity as indicated by the arrows (Fig. 1A). Scrotal magnetic resonance imaging revealed multiple solid nodules with the largest diameter being 18 mm in the right testis and 11 mm in the left. In T1A the nodules were hyperintense and in T2A they were hypointense. After intravenous gadolinium injection, intense homogeneous contrast accumulation was seen in the nodular lesions with contoured lobes and well-drawn borders (Fig. 1B, C). No pathological findings were visible in the computerized tomography of the abdomen.
Semen analysis showed oligoasthenoteratozoospermia. The patient's sperms were cryopreserved in case he underwent bilateral orchiectomy on the basis of malignant pathological findings. Because the testicular tumor could not be differentiated as malignant or benign on the basis of the laboratory and imaging findings, the patient underwent a right high inguinal testicular exploration. A 1.8-cm nodule was totally excised for frozen section analysis. Because the report of the frozen section analysis was benign, orchiectomy was not performed. After the tunica albuginea was sutured, the testis was placed back into the scrotum.
Histopathological analysis revealed that the cells forming the mass were similar to Leydig cells with separated fibrous tissue; significant, nucleolus, eosinophilic cytoplasm; and polygonal shapes forming in some areas nests and at other areas layers. Mitosis was rare and necrosis was not seen. The cell cytoplasmic fluid contained lipofuscin but no Reinke crystals. Immunohistochemical analysis revealed that the tumor cells totally diffused with vimentin and Melan-A but were focally immunopositive to inhibin and creatine. Placental alkaline phosphatase and Ae1/Ae3 were immunonegative and the tissue was defined as TART (Fig. 2A-C). The patient was diagnosed with TART, glucocorticoid treatment was initiated, and the patient was followed up.
DISCUSSION
The prevalence of TART changes in CAH patients. The incidence shows an increase according to tumor diagnosis and age. Moreover, TART is generally seen in insufficiently treated or untreated patients with CAH owing to the elevated ACTH levels. Hence, it is often detected in adolescents and young adults.
In the present case, 11β-hydroxylase deficiency-driven CAH had been diagnosed yet inadequately treated and followed up. The testicular masses were diagnosed when the patient was hospitalized for regulation of hypertension. Changes in the levels of 11-deoxycortisol to cortisol and 11-deoxycorticosterone to corticosterone were decreased owing to the defect in 11β-hydroxylase activity. A decrease in cortisol levels leads to ACTH stimulation and thus to growth in adrenal tissue and adrenal ectopic tissues [4].
TARTs are very difficult to differentiate from Leydig cell tumors (LCTs), which are mostly common in stromal testicular neoplasia leading likewise to precocious puberty and testicular masses [5]. The presentation of these two entities is the same, yet the therapeutic approaches differ. Whereas LCTs require surgical treatment, most cases of TARTs respond to steroid-suppressive therapy [5]. In the diagnosis of TART and malignant tumors, the use of magnetic resonance imaging and ultrasonography is beneficial yet not determinant. Although the initial evaluation of the present case was in favor of testicular malignancy (LCTs) or TART, for differentiation, biopsy results are considered to be conclusive.
TART can be diagnosed on the existence of LCTs. The clinical manifestations of TARTs are changes in blood pressure and bilateral tumors accompanied by a family history of TART. A CAH-positive family history is almost always prevalent. On the other hand is testicular malignancy manifest with recurrence and metastases. The bilateral presence of TART is determinant in diagnosis; however, 3% of bilateral masses consist of LCTs [6]. TART as well as LCT is generally evident in adolescents and young adults. Precocious puberty and gynecomastia might be evident in both; however, gynecomastia is more frequent in LCT [6,7]. The laboratory findings supporting TART are hypokalemia and normal tumor indicators such as βhCG, AFP, and LDH. In ultrasonography, TART is prevalent in the form of multiple hypoechoic nodules, whereas LCTs appear as single hypoechoic nodules [8]. The present case was a 16-year-old male patient with a history of hypertension and multiple bilateral lesions. Normal AFP, hCG, and LDH levels were found in the blood analysis. Although these findings suggest TART, a definitive diagnosis requires histopathological diagnosis.
Therefore, in the present case, a high inguinal testicular exploration with nodal excision was done to analyze frozen sections to determine the prospective treatment modality. In case the histopathological diagnosis was malignant and bilateral orchiectomy was thus unavoidable, cryopreservation was done before the procedure. Because the frozen section report was benign, orchiectomy was not performed.
The pathology report in the present case supported TART. After the procedure, the patient was enrolled into the follow-up protocol and referred to pediatric endocrinology for glucocorticoid treatment planning.
Although TART is not among the prevalent tumors, one of the most important problems is its differentiation from malignant tumors. Despite the fact that clinical, radiological, and biochemical indicators support the diagnosis, histopathological diagnosis is decisive.
In patients with CAH, early diagnosis and conservative treatment in TART patients is essential because a delayed radical approach will result in prospective infertility and testicular hypofunction. In the present case, clinical, radiological, and biochemical diagnoses supported TART; yet biopsy to make a decisive diagnosis could not be conducted.
In conclusion, to prevent irreversible testicular damage, early detection of TART is important. CAH patients should be regularly followed up for TART, and those with nodular testicular lesions should be well evaluated before any invasive treatment and diagnosis modalities are preferred by urologists.

 XML Download
XML Download