

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Psoas abscess is a rare disease with a subtle and often nonspecific presentation that frequently provides a diagnostic challenge [1]. In the early part of the 20th century, psoas abscess was mainly caused by tuberculosis of the spine; however, the decline in the prevalence of tuberculosis has led to the emergence of nontuberculous bacterial organisms as the principal source of psoas infection [2].
Genitourinary tuberculosis is the second most common form of extrapulmonary tuberculosis after peripheral lymphadenopathy [3]. Renal tuberculosis is slowly progressive, asymptomatic, and highly destructive, with instances of autonephrectomy of the kidney on diagnosis.
Recently, the author was presented with a 45-year-old woman with an autonephrectomized tuberculous kidney in which the pararenal abscess had spread to the ipsilateral psoas muscle. This was successfully treated with percutaneous drainage followed by nephrectomy and additional antituberculous medications. To my knowledge, a psoas abscess secondary to renal tuberculosis has been reported in only one previous article, written in Italian [4]. Here, a case of psoas abscess arising from renal tuberculosis is presented.
CASE REPORT
A 45-year-old woman presented with dull aching abdominal pain in the right upper quadrant over the past 2 months. The pain was vague in character and nonradiating. She did not complain of fever or chills. There were no gastrointestinal or urological complaints. She had a history of mycobacterial cervical lymphadenitis in her twenties, which had been treated with antituberculous medications for 2 years.
Her initial blood pressure was 120/70 mmHg and her body temperature was 36.6℃. A physical examination revealed a palpable mass in the right upper quadrant below the lower costal margin without obvious tenderness. No costovertebral angle tenderness was elicited. Initial hematological and biochemical tests showed no remarkable findings, except a decreased hemoglobin level (10.9 g/dL). Neither pyuria nor hematuria was shown in the urinalysis.
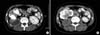
Abdominal plain radiography showed extensive lobulated calcifications on the right renal shadow, suggestive of a tuberculous kidney (Fig. 1). Abdominal computed tomographic (CT) scan better demonstrated calcifications of the right kidney, right upper ureter, and retroperitoneal lymph nodes. There was no functioning parenchyma in the right kidney, and the dilated calyceal spaces were filled with low-attenuation contents. These abscess-like intrarenal collections extended to the right psoas muscle through the right posterior pararenal space. A CT scan showed apparent thick-walled collections measuring 6 cm×4 cm×8 cm in the right psoas muscle (Fig. 2). A percutaneous catheter was placed in the right posterior pararenal space to obtain contents for culture and to drain the abscess. A purulent, light gray material was drained from the catheter; however, no acid-fast bacilli were seen in the pus, and the pus culture yielded no bacteria. The results of polymerase chain reaction (PCR) for Mycobacterium tuberculosis in the pus were also negative. The patient was explored and subjected to a right nephrectomy to surgically remove the infectious source. The remaining psoas abscess, which had degenerated into a hard mass, was also removed. The histopathological examination of the nephrectomized specimen and the specimen from the remaining psoas abscess revealed chronic granulomatous inflammation with caseous necrosis, consistent with tuberculosis (Fig. 3). No acid-fast bacilli were detected by Ziehl-Neelsen staining of the specimens. Postoperatively, the patient took antituberculous drugs for 6 months. The patient is now asymptomatic at 2 years of follow-up.
DISCUSSION
Most patients with renal tuberculosis are asymptomatic, and symptoms arise when there is a descending infection in the urinary bladder [5]. The paucity or nonspecificity of symptoms is an important cause of delayed diagnosis of renal tuberculosis. In this case, the tuberculous kidney itself must not have induced any discomfort, and it seems that it was not until development of the psoas abscess that the patient started to perceive symptoms.
In renal tuberculosis, the fibrosis can cause strictures in the calyceal stem or at the pelviureteral junction, which can result in the formation of chronic abscesses in the parenchymal tissue [3]. However, spreading of a tuberculous renal abscess to the pararenal space beyond Gerota's fascia is rare. In particular, a psoas abscess secondary to renal tuberculosis has been reported in only one previous article, written in Italian [4].
The clinical presentation of a psoas abscess is often variable and nonspecific. The clinical triad consisting of fever, back pain, and limp is present in only 30% of patients with a psoas abscess [6]. The patient in this case complained of only dull aching abdominal pain for 2 months. Although the patient had only vague symptoms, the diagnosis of the psoas abscess was relatively straightforward. A past history of tuberculous lymphadenopathy and the typical features on abdominal plain radiography provided an impression of renal tuberculosis. The CT scan, which was performed to further evaluate the renal tuberculosis, revealed abscess-like collections of the right psoas muscle extending from the posterior aspect of the right kidney, and thus the case could have initially been diagnosed as a psoas abscess secondary to renal tuberculosis. It should be noted that a previous history of tuberculosis can give an important clue to the diagnosis of genitourinary tuberculosis. Of course, to diagnose genitourinary tuberculosis or psoas abscess, a high index of suspicion in certain clinical settings cannot be overemphasized. The PCR test yielded a negative result in this case despite its high sensitivity and specificity for detection of tuberculosis. Multiple tests might have allowed the diagnosis of tuberculosis.
The cornerstone of antituberculous therapy is multidrug treatment, and it is currently being debated whether nonfunctioning tuberculous kidneys must be excised [7,8]. However, if a patient is symptomatic, then nephrectomy of a nonfunctioning kidney is usually mandatory. In this case, it was necessary to excise the right kidney with the adjacent degenerated abscess for the complete removal of the infectious source as well as for symptom relief.
It is usually recommended that surgical intervention for renal tuberculosis be delayed until antituberculous therapy has been administered for at least 4 to 6 weeks [7]. In this case, the examinations of the urine and the percutaneously aspirated abscess did not confirm the diagnosis of tuberculosis and preoperative antituberculous medical therapy was not done. Considering the clinical clues suggesting renal tuberculosis, however, preoperative antituberculous chemotherapy could have been justified for this patient. Although the antituberculous medication might not have effectively penetrated into the abscess, it could have reduced the chances of hematogenous spreading of tuberculosis during the operation. After confirmation of the pathologic diagnosis, the patient took antituberculous drugs for 6 months to lessen the relapse risk.


 XML Download
XML Download