

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Approximately one third of patients with renal cell carcinoma (RCC) have metastatic disease at the time of initial diagnosis (synchronous metastatic disease), and 40% to 50% will develop distant metastases after the initial diagnosis. Synchronous metastasis of RCC to the ureter or the bladder, however, is extremely rare.
CASE REPORT
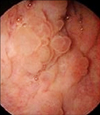
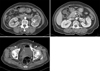
A 73-year-old woman complained of gross hematuria for the past 1 week. Her medical history and family history were negative for gross hematuria. Physical examination revealed no specific findings. Her serum creatinine on presentation was 0.4 mg/dL. Urine analysis showed numerous red blood cells. She underwent a cystoscopy that revealed a sessile mass on the right lateral bladder wall (Fig. 1). Abdominopelvic computerized tomography showed a 0.9 cm sized enhancing lesion on the right lateral bladder wall. A 6.4×5.3 cm sized heterogenous enhancing mass in the lower pole of the left kidney with left renal vein thrombosis, multiple small enhancing nodules in the pancreas parenchyma, and nodular thickening of both adrenal glands were also found (Fig. 2). Chest computed tomography (CT) showed hematogenous lung metastasis and left mediastinal and hilar lymph node metastasis. Transurethral resection of bladder tumor was performed for histological examination.
During the operation, the mass was found to be sessile, 1.0×1.0 cm in size, and with indistinct demarcation. Thus, the tumor was resected widely and its base was additionally resected. Pathological findings showed that the tumor base was free of tumor. The pathological analysis of the resected biopsy specimen revealed metastatic RCC of the clear cell type (Fig. 3). The patient underwent target therapy with Sorafenib 200 mg owing to the multiple metastatic sites. Five weeks after the target therapy, she fell down in the bathroom, sustained an intracranial hemorrhage, and died of accompanying hyponatremia and aspiration pneumonia.
DISCUSSION
Less than 2% of bladder cancers represent metastases from distant primary cancers [1,2]. Metastatic bladder cancers usually come from gastric adenocarcinoma, melanoma, and adenocarcinoma of the breast and colon. RCC is an uncommon source of bladder metastases, with fewer than 40 such reported cases. Such metastases may be synchronous or metachronous [3].
Frequent metastatic sites of RCC are the regional lymph nodes, lung, liver, bone, adrenal gland, brain, and skin. Reported metastatic sites in the genitourinary tract include the ipsilateral ureter, contralateral ureter, ureteric stump, bladder, and prostatic fossa [1,2].
Patients with RCC metastatic to the bladder typically present with gross hematuria. In the majority of cases, there is a well-established history of RCC. However, infrequently, the primary renal tumor may present initially as a bleeding bladder lesion [1,3]. In this case, the renal tumor was found during the staging work-up of the bladder cancer. Bladder lesions are generally sessile, spherical protuberances into the bladder lumen. In this case, the bladder tumor was sessile. Histological evaluation of the resected tissue is usually consistent with metastatic RCC. In this case, the pathological analysis of the resected biopsy specimen revealed metastatic RCC of the clear cell type.
The mechanisms underlying the spread of RCC to the bladder remain a matter of debate. Several possible mechanisms have been proposed, including hematogenous metastasis through the general circulation, retrograde spread of the tumor from the renal vein or renal hilar lymphatics down the periureteral veins or lymphatics that connect with pelvic organs, and direct intraluminal transit of tumor cells with seeding of the distal urothelium [1-6]. RCC commonly metastasizes through the bloodstream, leading to the synchronous discovery of a widespread area of metastasis. In this case, the multiple metastatic sites, including the regional lymph nodes, lung, bladder, adrenal gland, and pancreas, lend support to hematogenous metastasis through the general circulation.
Treatment options for RCC, particularly when metastatic, are limited owing to poor treatment response to chemotherapy and radiation therapy. Conventional surgical treatment remains controversial regarding the establishment of good criteria for its application and often results in poor treatment effects.
Before the development of target treatment agents, immune therapy had been widely used. Target therapy is now accepted as the standard therapy for metastatic RCC because of the superior effect of sunitinib and sorafenib, which target vascular endothelial growth factor receptor and platelet-derived growth factor receptor.
For cases in which RCC is metastatic at the time of diagnosis, as in this patient's case, the decision of whether to perform nephrectomy is debatable. For severe symptoms due to primary carcinoma, palliative nephrectomy can be performed, and nephrectomy is performed with an expectation of spontaneous regression or to improve the treatment effect and survival rate by reducing the total volume of primary carcinoma when systemic treatment such as immune therapy or chemotherapy is given. In doing so, careful consideration should be given to the patient's performance status, position and degree of remote metastasis, types and degree of differentiation of carcinoma cells, size of carcinoma, patient's age, and gender. For the treatment of metastatic lesions in the bladder, transurethral resection, partial cystectomy, and radical cystectomy have been used. Although genitourinary metastases are generally considered to have a poor prognosis, long-term survival is occasionally reported [6].
Prognosis has been reported to be good when only a single metastasis exists in the bladder, and follow-up without additional systemic treatment is possible after the surgical removal of the metastatic lesion in the bladder [7]. In addition, when carcinoma has metastasized to other organs at the time when RCC metastasis is found in the bladder, additional systemic treatment such as immune therapy is required.
In this case, considering the patient's performance status and the degree of remote metastasis, we decided that nephrectomy was not indicated. Thus, transurethral resection of the bladder tumor was performed and metastatic bladder cancer was confirmed. Chest and abdominopelvic CT and a whole-body bone scan showed adrenal and lung metastasis. Metastasis to the left mediastinal and hilar lymph node was also found. The patient was treated with target therapy with sorafenib owing to the multiple metastatic sites. However, she fell in the bathroom and suffered an intracranial hemorrhage that resulted in her death.

 XML Download
XML Download