

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mucormycosis is an opportunistic fungal infection that rarely occurs in immunocompetent individuals [1]. Isolated involvement of any organ is rare and only a few cases of renal mucormycosis have been reported [2-6]. We hereby report a rare case of renal mucormycosis with an atypical presentation in a healthy adult with no antecedent risk factors.
CASE REPORT
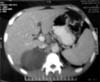
A 30-year-old normotensive nondiabetic male presented with complaints of right flank pain on and off for the past 1 year. The pain had started as a sudden severe aching pain that was initially associated with painless hematuria, low-grade fever, and nausea. The patient was admitted to the hospital and was managed on parenteral antibiotics. His symptoms subsided on this conservative treatment, but he continued to have similar recurrent episodes over the past 1 year. He had no history of decreased appetite or weight loss. On evaluation, the patient was found to have a total leukocyte count of 9,700 cells/mm3 and serum creatinine of 0.88 mg/dL. Urine examination was unremarkable. Contrast enhanced computed tomography revealed a right upper polar heterogeneous nonenhancing mass about 8 cm×10 cm in size (Fig. 1). The right kidney was found to have a glomerular filtration rate of 7.4 mL/min on a technetium 99m-diethylene triamine pentaacetic acid scan. The patient underwent a right nephrectomy, and histopathology of the resected specimen revealed necrotizing granulomatous inflammation associated with mucormycosis and xanthogranulomatous pyelonephritis (Fig. 2). Inflammatory cells consisted of foamy histiocytes, few multinucleate giant cells, plasma cells, and lymphocytes. Large areas of necrosis were present along with palisading epithelioid cells and epithelioid cell granulomas at the periphery. Fungal elements were described as broad, aseptate fungi with right angled branching hyphae (Fig. 3). The patient had an uneventful postoperative course and recovery. Because the patient showed no signs of sepsis preoperatively or postoperatively, no antifungals were given and the patient was managed conservatively on that front.
DISCUSSION
Zygomycosis is an opportunistic fungal infection that seldom occurs in individuals with a competent immune system [7]. The disseminated form accounts for approximately 9% of cases of mucormycosis; the organ most commonly involved is the lung. Involvement of the kidneys has been reported in up to 20% of cases with disseminated forms [8]. Involvement of single organs such as bone, heart, and kidney is rare. Gupta et al. [9] found 8 isolated cases of renal mucormycosis among 18 cases of disseminated disease. Renal transplant recipients with concomitant diabetes mellitus are most susceptible to renal mucormycosis. The mortality of different forms of mucormycosis reaches 75% to 100% in most series. Survival for isolated renal zygomycosis is estimated to be 65% [3].
The pathogenesis of renal mucormycosis is not clear. Hematogenous dissemination to the kidneys and retrograde spread from lower urinary tract infection have also been suggested [10]. Mucormycosis is characterized by the uniform presence of extensive angioinvasion with resultant vessel thrombosis and tissue necrosis. Both small and large arteries exhibit hyphal invasion and consequent thrombosis that leads to massive cortical and medullary infarction [8].
Most reports are cases with a predisposing factor such as AIDS, diabetes, drug abuse, or organ transplantation. Isolated renal mucormycosis has rarely been reported in healthy adults with minimal constitutional symptoms. Clinically, most patients with isolated renal mucormycosis present with fever, flank pain, tenderness, gross hematuria, or pyuria [2-6]. Renal failure is usually the result of near total occlusion of the renal arteries or their branches.
Our case was further documentation of isolated renal mucormycosis in a healthy immunocompetent adult. The patient had an atypical presentation in that he had no identifiable risk factors. Also, the patient had an indolent course with minimal constitutional symptoms contrary to the fulminant and aggressive course encountered in previous case reports. It is widely agreed that renal mucormycosis requires aggressive treatment including a parenteral antifungal such as amphotericin B followed by early nephrectomy. Because our patient was not toxic and had minimal constitutional symptoms, we decided that he did not require any additional treatment with antifungals. The patient has been asymptomatic for the past 9 months. We therefore hypothesize that immunocompetent, afebrile, nontoxic patients with a coincidental finding of renal mucormycosis in a nephrectomy specimen can do away with administration of nephrotoxic drugs such as amphotericin and can be managed with nephrectomy alone.


 XML Download
XML Download