

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Exstrophy of the bladder is a rare congenital anomaly. With the development of new techniques for repair, the quality of life of patients with exstrophy of the bladder has been markedly improved. However, it is now well recognized that exstrophy of the bladder is associated with an increased risk of bladder cancer. Here we present a case in which squamous cell carcinoma developed in the exstrophied bladder mucosa.
CASE REPORT
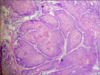
The patient, a 36-year-old woman with a known case of exstrophy of the bladder had undergone repair of the defect 17 years previously. However, dehiscence of the repair had occurred and the patient continued to leak urine from the lower abdominal wall. Six months following this, an ileal conduit urinary diversion was done to prevent the continuous leakage of urine. Six month prior to presentation, the patient had noticed an irregular mass arising from the exposed bladder mucosa that was rapidly increasing in size. On examination, a hemispherical growth with an irregular surface was seen in the region of the exposed bladder mucosa (Fig. 1). The computed tomography scan showed a mildly enhancing nodular lesion on the right side of the lower abdomen superficially. The lesion was confined to the urinary bladder. A wedge biopsy was taken from the growth, and the results were suggestive of squamous cell carcinoma. The results of a routine hematological evaluation, liver function tests, and a chest radiograph were normal. The patient thus underwent removal of the urinary bladder along with a cuff of the surrounding abdominal wall and pelvic lymph node dissection (radical cystectomy). After resection, there was a full thickness defect of the lower abdomen about 8 cm×9 cm in size. To cover this defect, the peritoneum was mobilized on both sides and was sutured in the midline. Both recti were also mobilized and sutured in the midline. The skin defect was resurfaced with an extended groin flap from the left side and the secondary defect thus created was covered by a split thickness skin graft (Figs. 2, 3). Histopathological examination of the resected specimen was suggestive of well-differentiated squamous cell carcinoma infiltrating the underlying muscle (stage pT2a) with dense lymphocytic infiltration of the stroma. All the resected margins and deeper plane of resection were free of tumor (Fig. 4). In the postoperative period, the patient developed a small collection beneath the flap that was drained by removal of two stitches, and daily dressings were done. This site granulated well and healed without any significant additional scaring. The patient is on regular follow-up and is doing well without any evidence of recurrence to date (5 months postoperatively) (Fig. 5).
DISCUSSION
Exstrophy of the bladder is a rare congenital anomaly, with an estimated incidence of 1 in 50,000 live births. It is more common in males (male:female, 5:1 to 6:1) [1]. Currently, exstrophy of the bladder can be diagnosed antenatally with the use of high-resolution real-time ultrasound. With advances in pediatric medicine and reconstructive surgery, the morbidity and mortality associated with this disease has decreased drastically. In the developing world, however, one may come across these patients at an older age, because there is often a delay before they seek medical advice. This was the case with our patient.
The malignant potential of exstrophied bladder mucosa is well known. Chronic irritation and infection leading to metaplastic transformation of the urothelium resulting in malignant changes is the most likely possibility. Adenocarcinoma is the most common type in cases of exstrophy of the bladder, accounting for 95% of cases, whereas squamous cell carcinoma accounts for only 3% to 5% cases [2-4].
The treatment of squamous cell carcinoma of the urinary bladder remains similar to the treatment of transitional cell carcinoma [5]. The gold standard of treatment of squamous cell carcinoma of the bladder is radical cystectomy, with no established guidelines for any adjuvant or neoadjuvant therapy [6,7]. Radiation therapy is offered to inoperable cases or those who refuse surgery. In our case, radical cystectomy was done. The histopathological examination report confirmed the localized disease; thus, no consideration to chemo-radiation was given.
There are no specific guidelines for follow-up in cases of squamous cell carcinoma. The guidelines for follow-up of bladder cancer in general are applied also for patients with squamous cell carcinoma. Slaton et al. [8] recommended annual screening with a physical examination, measurement of serum chemistry indexes, and chest radiograph for patients with pT1 disease; semiannual evaluation for patients with pT2 disease; and quarterly evaluation for patients with pT3 disease. For the last group, a semiannual computed tomography scan was also recommended.
Repair of the abdominal wall defect created is also an issue when dealing with such cases, because repair under tension may lead to wound dehiscence and accompanying morbidity. The results are cosmetically inferior in such cases. The use of mesh for the repair for abdominal wall defects has been well described. Another method is the use of a tensor fascia lata flap [9]. In our case, because the defect was smaller, it was covered by mobilizing the rectus sheath on both sides, and skin coverage was done with the extended groin flap. The help of plastic surgery colleagues may be sought when closure of the defect is done. We obtained the help of plastic surgeons our case as well.
The prognosis of squamous cell carcinoma of the bladder is reported to be poor with an advanced stage at detection. Kassouf et al. [10] reported a 2-year overall survival of 47.6% with a median recurrence-free survival of 5.1 months.
In conclusion, the fact that exstrophy of the bladder is a predisposing factor for the development of bladder malignancies is well known. Adenocarcinoma is the usual type of malignancy in such cases. Squamous cell carcinoma contributes to only a minority of cases. Treatment of such cases, especially the reconstructive part, is difficult, but good results can be obtained in patients who present early with localized disease, especially when a multidisciplinary approach to treatment is adopted.




 XML Download
XML Download