

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Malignant melanoma constitutes approximately 4% to 5% of all newly diagnosed cancers, with 68,130 cases per year in the United States [1]. Even though malignant melanomas have been observed to metastasize to virtually every tissue, certain organs such as liver, lung, brain, and heart are clearly favored in terms of frequency [2]. Metastasis of malignant melanoma to the prostate is extremely rare in clinical practice, and to our knowledge this is only the second case report in the literature.
CASE REPORT
A 50-year-old male presented with complaints of lower urinary tract symptoms (LUTS) for 6 months and painless gross hematuria for 2 months. The results of a physical examination were completely normal, except for prominent prostatic enlargement detected by digital rectal examination. Three years ago he had been diagnosed as having malignant melanoma after a left axilla mass biopsy and had undergone wide local excision and left axillary node dissection. He was well for 2.5 years with a complete response to interferon treatment until his LUTS had started 6 months ago.
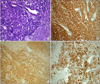
Positron emission computed tomography screening of the body showed increased metabolic activity around the prostatic gland, and pelvic magnetic resonance imaging revealed a 10 cm×4 cm×8 cm prostatic mass lesion that displaced the rectum posterior and the sigmoid colon laterally (Fig. 1A, B). Transrectal ultrasound-guided prostate biopsy was performed to rule out prostatic cancer and to diagnose the mass, although the prostate-specific antigen level was 0.2 ng/mL, which is consistent with a benign prostatic gland. The pathological diagnosis was reported as malignant melanoma infiltration of the prostatic gland. The patient subsequently underwent transurethral resection of the prostatic gland for symptomatic relief, and after resection of the normal prostatic gland layer, melanoma tissue was seen (Fig. 2). Pathologic examination with immunostaining with S-100, HMB45, and melanin-A confirmed the diagnosis of malignant melanoma (Fig. 3). At 6 months after the surgery, the patient died because of uncontrolled metastases of the melanoma to the liver and lung.
DISCUSSION
Metastatic neoplasms of the prostate are extremely rare and represent 2.1% of all prostate tumors. Secondary tumors can spread directly to the prostate from the bladder and rectum. The most common primary sites of metastases to the prostate are the lung and pancreas, and there are isolated examples of metastases from the bladder, rectum, skin (malignant melanoma), breast, eye (malignant melanoma), adrenal cortex, and gall bladder [3].
The biological behavior of malignant melanoma is very unpredictable, and variations in metastatic spread are well known in clinical practice. The genitourinary tract is a common site of metastasis from malignant melanoma and may be involved in as many as 37% of cases according to autopsy series. Metastases in the pelvic area occur mainly in reproductive organs including the ovary, testis, prostate, bladder, and pelvic lymph nodes. There are a few well documented cases of primary malignant melanoma of the prostate in the English literature, and most cases attributed to the prostate actually originate from the prostatic urethra [4]. Grignon et al. [5] reported a case of malignant melanoma with metastasis to adenocarcinoma of the prostate. In our case, the patient was completely well for 2.5 years after the diagnosis of malignant melanoma and had a complete response to interferon treatment until his LUTS started. Patients with secondary tumors of the prostate are usually symptomatic, presenting with prostatism, hematuria, or pelvic pain, and are almost always those with widely disseminated disease. Owing to its infrequency, primary malignant melanoma or metastasis of malignant melanoma to the prostate presents a difficult diagnostic and management challenge. The diagnosis of prostatic malignant melanoma depends on transurethral resection of the prostate and careful histopathologic evaluation. Melanoma tumor cells are stained with Melan-A and also with HMB45 and S-100. Metastatic malignant melanoma cells usually exhibit variable expression of the common melanoma-associated antigens. In some instances, this variability can create a diagnostic dilemma in which case-special immunostain is useful. These include antibodies to gp100, MART-1/Melan-A, and other melanoma antigens [6].
Treatment of patients with systemic melanoma should include careful evaluation for the potential role of surgery, radiotherapy, and systemic therapy, i.e., chemotherapy and immunotherapy [7]. Transurethral resection of the prostate can improve LUTS and hematuria. Radical prostatectomy seems to be the treatment of choice in potentially curable patients with solitary metastases. Unfortunately in this case, after the transurethral resection of the prostate, metastasis to the lung and liver was detected, which demonstrates the aggressive natural history and poor prognosis of this disease. The main use of chemotherapy in metastatic malignant melanoma patients remains palliative. Some chemotherapy regimens can produce objective responses; such regimens have not demonstrated improved survival [8]. Malignant melanoma is particularly susceptible to immune modulation, and numerous immunotherapy strategies including interferon-alpha, melanoma vaccines, and interleukin-2 have been used for treatment.
Despite new treatment options, the survival rate of patients with metastatic malignant melanoma has not changed significantly over the past three decades, and the prognosis of these patients remains dismal. From the literature, the overall median survival of patients with systemic metastasis from malignant melanoma is about 6 to 7.5 months; the estimated 5-year survival rate is 6% [9]. Survival is dependent on the sites of first metastases, the resectability of the metastases, and the number of metastases. Our presented patient was well for 2.5 years and had a complete response to interferon treatment until prostatic metastasis occurred. After that, the malignant melanoma metastatised to the liver and lung and the patient died within 6 months.


 XML Download
XML Download