

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aphallia is a rare congenital anomaly with an estimated incidence of 1 in 10 to 30 million births, and around 60 cases have been reported so far [1]. Definitive management involves phalloplasty and urethral reconstruction, which is surgically challenging but is associated with good outcomes [2]. The major drawbacks of phalloplasty are the urethral complications and problems with penile stiffeners. Regular follow-up is essential for early detection of urethral complications such as urethral stricture, urethral stenosis, and urethral fistula [3]. Urethral hairballs have occurred in patients who have undergone hypospadias repair following urethroplasty with the use of a skin flap for repair and are particularly troublesome owing to their recurrent nature. To the best of our knowledge, this is the first case report of a "tricholithobezoar," which is the formation of a stone over a hairball, as a complication after phallic and urethral reconstruction in a patient with aphallia. Herein, we describe the clinical presentation, management, and prevention of such an unusual complication.
CASE REPORT
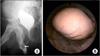
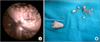
An 18-year-old man born with aphallia had undergone phallic reconstruction in childhood at the age of 13 years, which was followed by total urethral reconstruction with a buccal mucosal graft and groin-based pedicle (Singapore) flap. The patient had 5 years of regular follow-up after his urethral reconstruction. In the present case, he presented with a gradual onset of thinning of his urinary stream for 6 months followed by acute urinary retention. Examination revealed a firm swelling in the perineum over the reconstructed urethra. Urethral catheterization to relieve the acute retention was unsuccessful and hence an emergency suprapubic cystostomy was performed. The results of a voiding cystourethrogram revealed a filling defect in the distal urethra (Fig. 1A). On urethroscopy, a solitary, smooth 3 cm×2 cm sized stone was seen in the dilated urethra (Fig. 1B). Pneumatic lithotripsy was used initially to fragment the stone, but owing to its resistant nature (because of the presence of hair in the stone interstices) (Fig. 2A), the stone could not be fragmented completely. A bulbar urethrotomy was therefore performed to remove the remaining bezoar (Fig. 2B). Following removal of the tricholithobezoar, hair from the anterior urethra was mechanically epilated. The urethrotomy was closed primarily. The postoperative period was uneventful and patient could successful void with a peak flow rate of 16 mL/s.
DISCUSSION
A tricholithobezoar, or the formation of a stone over a hairball, is an unusual complication and has been seen when a hair-bearing skin flap is used for urethral reconstruction, such as in hypospadias repair [4,5], and during inadvertent introduction of hair into the bladder during catheterization or clean intermittent catheterization, especially in a paraplegic patient [6,7]. In our case, the phallic reconstruction was done with a neurovascular pudendal-thigh flap (Singapore flap). This hair-bearing skin flap led to periodic shedding of hairs in the redundant urethra. The hair acted as a nidus and along with other aggravating factors, such as stasis of urine in the dilated and sacculated urethra, recurrent urinary tract infections, and the lithogenic potential of urine, led to tricholithobezoar formation.
These stones present as gradually increasing painless lumps with obstructive urinary symptoms when present in the urethra and with recurrent episodes of urinary tract infections when present in the bladder. A plain radiograph will show characteristic serpiginous radio-opacity and an intravenous urogram will show a filling defect in the bladder [7]. In our case, a plain X-ray was not done because only stricture and stenosis of the neourethra remained as part of the differential diagnosis. However, the voiding cystourethrogram showed a filling defect in the urethra that on urethroscopy was confirmed to be a stone.
The management of this case was challenging because the stone was located in the surgically reconstructed neourethra and was difficult to fragment owing to the presence of hair in its interstices. Open urethrolithotomy or endoscopic urethrolithotripsy have been used to treat such stones with complete clearance. In our case, pneumatic lithotripsy was performed to debulk the bezoar followed by urethrotomy, which helped in its complete removal and minimized the size of the urethrotomy.
Elective epilation can be a prophylactic measure to prevent tricholithobezoar formation. Gallium-aluminum-arsenate (GaAlAs) diode laser (wavelength 810 nm; at a power of 15 W for 2 seconds) through a side-firing laser fiber has been used in multiple sessions to destroy the hair follicles [8]. A dilute solution of thioglycolate has also been used to prevent recurrent hair growth but has met with limited success [8]. In the series by Lumen et al. [3] comparing a free radial forearm flap with a pedicled anterolateral thigh flap, 8 of 11 patients with phalloplasty underwent urethral reconstruction, and after a mean follow-up of 25 months, none of the patients developed such a complication. This could be due to the relative absence of hair in the free radial forearm flap, thus favoring its use to prevent such an unusual complication. Mechanical epilation by plucking of hairs can also be done whenever feasible, as in our case.
In conclusion, patients with urethral reconstruction using a groin skin flap can present with the long-term complication of a tricholithobezoar. This case highlights the need for prophylactic removal of hairs along with long-term follow-up to detect such an unusual complication.
 XML Download
XML Download