

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although renal pelvic stones larger than 20 mm in size are treated by percutaneous nephrolithotomy (PCNL), they can be directly removed by pyelolithotomy. Direct removal by pyelolithotomy is especially indicated in cases of failed extracorporeal shock wave lithotripsy (SWL) or endoscopic removal and in patients with anatomical variations in the location or shape of the kidney; concomitant abnormalities, including ureteropelvic junction obstruction; and urinary infections needing definitive clearance of calculi [1,2]. Although open pyelolithotomy is possible, laparoscopic surgery is preferred because it is less invasive. Since the first laparoscopic nephrectomy [3], laparoscopic surgery has been proven to have several advantages over open surgery. Nowadays, laparoscopic surgery is increasingly being used as a standard operation in many urologic procedures [4]. The primary objectives of attempts to further develop laparoscopic techniques and instruments are reductions in operative morbidity and improved cosmesis, which has led to the development of laparoendoscopic single-site (LESS) surgery.
LESS surgery is one of the advancements in the field of urology. This procedure has gained popularity over other techniques because it requires a smaller incision, which helps to improve postoperative recovery and cosmesis [5,6]. Herein, we present our initial experiences with four patients who underwent transumbilical LESS pyelolithotomy for the treatment of large stones in the renal pelvis. For the procedures, we used a Carter-Thomason (CT) needle grasper instead of an additional port.
MATERIALS AND METHODS
Between October 2010 and November 2011, LESS pyelolithotomy was performed in four patients (one woman and three men). The mean age of the patients was 57.8 years (range, 39 to 71 years), and their mean body mass index was 23.01 (range, 18.42 to 26.99). Our patients were free to choose any operative method. All operations were performed by a single surgeon. Preoperative laboratory tests and radiologic studies, including nonenhanced computed tomography, were performed. One patient had previously undergone an open adrenalectomy. Urinalysis showed that all patients had hematuria and pyuria. The characteristics and perioperative outcomes of the patients are presented in Table 1.
1. Technique
A double-J ureteral stent was inserted preoperatively (Fig. 1), and the operation was performed transperitoneally. The patient was positioned in a 70° lateral position. A homemade single-port device, made by using a size-6 surgical glove and a small-sized Alexis wound retractor (Applied Medical Resources Co., Rancho Santa Margarita, CA, USA), was inserted into the peritoneal cavity through a 2.5-cm periumbilical incision. One 5-mm and two 11-mm trocars were inserted into the glove of the homemade port and were fixed by using rubber bands. Carbon dioxide insufflation was used to maintain an intraperitoneal pressure of 14 mmHg, and a 10-mm 30° laparoscope (EndoEYE, Olympus Co., Tokyo, Japan) was inserted into the peritoneal cavity. The operation was performed by using standard 5-mm and 10-mm laparoscopic instruments, ultrasonic scissors (SonoSurg, Olympus Co.), and 5-mm articulating instruments (Cambridge Endo, Framingham, MA, USA).
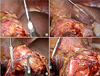
The LESS procedure replicated the procedure used in open ureterolithotomy (Supplementary data). The ureter was identified in the retroperitoneal fat medial to the psoas muscle and was traced to the renal pelvis. The stone was palpated in the renal pelvis, which was dissected to release the adhesions. A needle grasper from the CT needle suture device (Inlet Medical, Eden Prairie, MN, USA) was inserted in the peritoneal space at the subcostal margin; the tip of the device was covered with a plastic cap (Fig. 2). The device was used to manipulate the liver, spleen, and kidney. The pelvis was incised longitudinally; the incision was started by using a hooked blade and was continued by using laparoscopic scissors. The stone was removed with laparoscopic forceps. If a large stone adhered to the pelvic wall or extended to the calyx, it was gently rotated by using 10-mm laparoscopic forceps to facilitate its extraction. Running 4-0 Vicryl sutures were placed to achieve watertight closure of the pelvis. The previously placed double-J stent was left in situ. The CT needle grasper, without a cap, was useful for grasping the suturing material. After completion of the suturing, the stone was removed, and a Jackson-Pratt drain was placed and fixed through the periumbilical incision (Fig. 1).
These extracted stone samples were analyzed by using a modified Hodgkinson's method [7]. We retrospectively analyzed all data, including the operative results.
RESULTS
All LESS ureterolithotomies were completed successfully without conversion to conventional laparoscopic or open surgery; no additional ports were needed. One patient underwent simultaneous transurethral resection of the prostate.
The mean operative time was 124.5 minutes (range, 80 to 157 minutes). The mean estimated blood loss was 255.2 mL (range, 120.0 to 549.9 mL). There were no significant complications, except in one patient who required transfusion because he underwent simultaneous transurethral resection of the prostate. Postoperative pain control was achieved by using patient-controlled analgesia with 40 mg of morphine and 150 mg of ketorolac for 2 days. Additional pethidine injections were administered to two patients. The mean duration of hospital stay was 8.3 days (range, 5 to 11 days).
The stones were located in the renal pelvis; one patient had a large stone occupying the renal pelvis and lower pole. The mean diameter of the stones was 3.9 cm (range, 3.0 to 5.1 cm). Chemical analysis of the stones showed that three patients had calcium-containing stones and one patient had a uric acid stone (Table 1). Postoperative radiologic study showed no remnant stones in the renal pelvis. The stone clearance rate was 100%.
DISCUSSION
Pyelolithotomy is one option for treating complicated cases of large renal pelvic stones. It may be indicated in cases in which PCNL and SWL are not available. It affords a high chance of complete stone removal even with large stones and corrects a concomitant ureteropelvic junction obstruction [1,2]. Continuous advancements in laparoscopic surgery may lead to laparoscopic pyelolithotomy (LPL) becoming a feasible modality for the treatment of renal pelvic stones. LPL duplicates open surgery but with the advantage of minimal invasiveness [8]. The indications are the same as for open surgery. In the selection of LPL, surgeons should consider the characteristics of the laparoscopy. In particular, LPL can provide a magnified image to identify aberrant vessels and vascular injury. Although it is technically difficult to complete sutures in the case of a huge renal pelvis, LPL allows easy detection of the obstruction site.
Gaur et al. [9] presented 8 cases of retroperitoneal LPL. Although their success rate was low (62.5%) because of their inexperience and the unavailability of instruments, they recommended the use of laparoscopic suturing techniques and placement of double-J stents. Jordan et al. [10] also had performed an LPL procedure by using a transperitoneal approach in a 16-month-old child. Successful cases after these initial reports suggest that LPL can be used as an alternative to PCNL. Kramer et al. [11] performed LPL with a transperitoneal approach in five patients who had renal anomalies such as horseshoe and pelvic kidneys. However, Goel and Hemal [12] reported that LPL had a longer operative time and convalescence period, was more invasive, and had less cosmetic advantage. They concluded that LPL should be performed in patients who require adjunctive procedures or have urinary anomalies. In their study of LPL with the retroperitoneal approach and SWL, Chander et al. [13] showed that LPL resulted in better stone clearance, fewer hospital visits, and a lower analgesic requirement. They concluded that the main cause of the lack of popularity of LPL was its steep learning curve.
Minimally invasive approaches have been developed in laparoscopic surgery. Laparoscopic surgery involving a single incision and multi-lumen ports is one such procedure [14,15]. LESS surgery yields superior cosmetic results and shows faster recovery than the standard laparoscopic surgery in a large-volume center [16]. Choi et al. [17] reported LESS ureterolithotomies with the use of a homemade single-port device, a double-J ureteral stent, and intracorporeal sutures. Wen et al. [18] reported 10 cases of LESS ureterolithotomies through the retroperitoneal approach and compared these with conventional laparoscopic ureterolithotomy. They found no difference in operative time, estimated blood loss, or postoperative analgesic duration. Cosmetic results were superior in the LESS group according to both the study nurses' and the patients' assessments.
However, we could not find any reports describing LESS pyelolithotomies in a large series with technical details of the procedure. We assume that LESS pyelolithotomies may be uncommon for several reasons. It is difficult to dissect around the renal pelvis because of adhesions from inflammation and the risk of damaging the major blood vessels. Moreover, intracorporeal suturing is difficult to perform and may require an additional port. Finally, PCNL is an existing effective method for treating large renal pelvic stones. Despite these limitations, we have performed LESS pyelolithotomy and found that it increases the stone clearance rate, is minimally invasive, and offers cosmetic advantages.
We found that LESS pyelolithotomy showed acceptable operative results, including complete stone clearance, that were comparable to those of conventional laparoscopy. However, one patient required blood transfusion because of technical difficulty in dissecting the renal pelvis, which showed abundant perirenal fat and adhesion; moreover, this patient underwent a simultaneous transurethral resection of the prostate. The mean duration of hospital stay was longer than that previously reported for LPL because the medical insurance system of our country differs from the insurance systems in other countries.
The LESS technique that we used has certain distinguishing operative features. We used a homemade single-port device with three channels of an 11-mm trocar for the right hand of the operator, an 11-mm trocar for the camera holder, and a 5-mm trocar for the left hand of the operator. Although it took time to make the device and insert it into the peritoneal cavity, and there was a possibility of tearing during insertion of the instrument, the device itself was developed at a low cost and provided high flexibility [19]. The broad range of instrumental movement possible because of the flexibility of the device enabled us to perform the laparoscopic intracorporeal suture by using a rigid needle holder.
The CT needle suture device consisted of a 5-mm, 10-mm, or 12-mm cone; a sharp needle; and a single-action grasper. It has been used for closure of the fascia incision at trocar sites. Elashry et al. [20] showed that the CT needle suture device facilitated the fastest trocar wound closure with 100% intraoperative success. We used it for LESS surgery. It could be inserted through a skin puncture without an incision. There was no change in the puncture site in the operation. A cap of a 20-gauze needle and a short segment of fluid line attached to the grasper were useful for manipulating the organs to clear the operative field. It was often used as a retracting instrument for liver, spleen, kidney, and bowel. For facilitating the suture, the grasper without the cap was used to hold the suture material. After removal of the device, the insertion site did not require fascial or skin closures.
Our study had several limitations. While performing this small pilot study of our technique, we did not obtain enough cases and data to compare LESS pyelolithotomy with SWL or PCNL. Further surgical experiences and longer follow-ups are needed to evaluate the benefits of this technique with respect to cosmesis and convalescence and to compare the findings with those obtained for open or laparoscopic pyelolithotomies.
CONCLUSIONS
Although our study had certain limitations, our findings indicated that LESS pyelolithotomy with the use of a homemade port and a CT needle grasper can be a feasible treatment modality for large renal pelvic stones. Compared with open or laparoscopic pyelolithotomies, LESS pyelolithotomy is less invasive and has greater cosmetic advantages. The CT needle grasper was useful for resolving the technical difficulties involved in the LESS surgery without an additional trocar.


 XML Download
XML Download