

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Primary ureteral tumors are classified as being of epithelial or mesodermal (nonepithelial) origin. Epithelial tumors are mainly urothelial carcinoma, and mesodermal tumors are represented by fibroepithelial polyps. In the Korean literature, 20 giant ureteral polyps over 1 cm in size have been reported. The presence of polyps in the urinary tract is rare, and the malignant potential of benign polyps is very low [1,2]. Here we describe the first case of urothelial carcinoma arising from a large ureteral polyp in the Korean population.
CASE REPORT
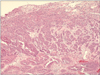
A 50-year-old man presented with a mass in the bladder that was detected during a routine checkup. He experienced intermittent gross hematuria. He had no history of flank pain, urinary tract infection, or urothelial carcinoma. The results of a physical examination, urinalysis, routine blood tests, and urine cytology were normal. Computed tomography (CT) showed a filling defect and a mass in the left distal ureter without hydronephroureterosis (Fig. 1). Cystoscopy showed a polypoid mass protruding from the left ureteral orifice with periodic movement and with an edematous, hyperemic mucosal lesion at its end (Fig. 2). A cystoscopic biopsy revealed urothelial carcinoma, of the nested variant, at the top of the polyp (Fig. 3). With the patient under general anesthesia, the remaining mass was removed by ureteroscopy and the base of the mass was subjected to frozen section analysis. The margin at the base of the mass was clear (asterisk in Fig. 4A). The resected mass had a long, smooth-surfaced stalk with an erosion site at the tip from the previous biopsy site (arrow in Fig. 4A). The polyp was covered by normal urothelium and the core was composed of a loose edematous and vascular stroma (Fig. 4B). There were no remaining carcinoma cells in the remnant polypoid mass. There was no evidence of recurrence on the physical examination, cystoscopy, urine NMP22 level, or CT conducted 3 months postoperatively.
DISCUSSION
Fibroepithelial ureteral polyps are rare benign tumors in the ureter. Most cases occur between the second and fourth decades of life; such tumors are rare in children and in the elderly [3,4]. The etiology of ureter polyps is thought to be congenital or acquired with exposure to chronic irritants, such as stones, infection, and inflammation. Ureteral polyps accompanying urolithiasis have been found in some cases [5]. The most common presenting symptoms are intermittent or recurrent flank pain and hematuria. Lower urinary tract symptoms such as frequency and dysuria are less common [6]. Ureteral polyps are usually located in the renal pelvis and upper ureter. They more commonly involve the left side (65%, 15/23, two cases were bilateral) and proximal ureter (72%, 18/25) in the Korean population. They are most often a single, unilateral polyp. Sometimes they can be bilateral or there may be multiple polyps. Kim et al. [7] reported a bilateral case with over 20 small polyps in the mid-upper ureter. The patients present with either hematuria or flank pain secondary to partial ureteral obstruction. However, if the polyp can move in and out with the urine flow, there may be no symptoms or signs of urinary tract obstruction, as in our case.
The risk of malignant transformation of ureteral polyps is very low. Only two fibroepithelial polyps with urothelial carcinoma and one fibroepithelial polyp with carcinosarcoma have been reported [1,2,8]. Ours is the first case in the Korean population. Because the results of urine cytology tests can be false-positive and the gross appearance can be hard to distinguish accurately, it is difficult to make a correct diagnosis preoperatively. In fact, the results of urine cytology were positive in two of the seven reported cases [5,9]. Given the low risk of malignancy, the traditional treatment of ureter polyps is segmental resection with or without endoscopy. Ureteroscopy is a useful technique for diagnosing and treating ureteral polyps. Recently, some studies have reported primary endoscopic polypectomy [10]. If patients have severe hydronephrosis, decreased renal function, or stones, conventional surgery can be considered [5].



 XML Download
XML Download