

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Imaging methods may be more accurate than physical examination in determining which organs are involved in pelvic organ prolapse. General landmarks for imaging procedures allow comparisons with other imaging studies and the physical examination. These landmarks are as follows: 1) the lower edge of the symphysis, to which high priority should be given; 2) the superior edge of the symphysis; 3) the ischial spine and tuberosity; 4) the obturator foramen; 5) the coccyx; and 6) the promontory of the sacrum. For many years, the use of contrast radiography dominated in the evaluation of the lower urinary tract. The obligatory method included the following information: projection, type and amount of contrast media, any urethral appliance used, and type of exposures. Reports in the 1980s showed ultrasound examination to be a valuable alternative to radiology that additionally provides a continuous visualization of dynamic events, but at that time there was still no standard in urogynecologic sonography.
In August 1995, the German Association of Urogynecology organized a consensus meeting on urogynecologic sonography and drew up the "Recommendations of the German Association of Urogynecology on Functional Sonography of the Lower Female Urinary Tract" [1]. According to them, there are two different techniques: 1) endosonographic applications, such as vaginal and rectal sonography (5 to 7.5 MHz frequency), and 2) external applications, such as perineal (3.5 to 5 MHz frequency), introital (5 to 7.5 MHz frequency), and transabdominal sonography.
The purpose of the present study was to compare the ultrasound characteristics of patients with concomitant urinary stress incontinence (USI) and genital prolapse (GP) with those of patients with isolated USI. The hypothesis was that the mobility of the bladder neck (BN), as evaluated by use of different ultrasound parameters, would be greater in the dorsal and caudal direction in patients with isolated USI than in those with concomitant USI and GP.
MATERIALS AND METHODS
Eligibility criteria for participants were as follows: presence of USI with or without GP stage I or II (according to the pelvic organ prolapse quantification [POP-Q] system) [2]. The data were collected at the Department for Urogynecology and Pelvic Floor Disorders in the Clinic of Gynecology and Obstetrics, Medical Faculty of the "Saint Cyril and Methodius" University in Skopje from 1 January 2010 to 31 December 2010. The study was designed according to the CONSORT statement [3].
The experimental arms were as follows: 1) coexisting GP stage I/II and USI, i.e., the USIGP group (n=136), and 2) presence of USI without GP, i.e., the USI group (n=132). The study was approved by the local research ethics committee of the Macedonian Association of Gynecologists and Obstetricians. All ultrasound examinations were performed by the author of this article. The study was a prospective observational study with no allowance for patient preference.
Every postmenopausal patient with isolated USI or USI and GP stage I/II admitted to our department in the above-mentioned period was assessed for eligibility (n=278). Ten patients were excluded from the study because they were unwilling to participate. Thus, 268 patients were randomly assigned, and all of them completed the study. After they underwent a complete urogynecologic examination according to the Urogynecological Protocol [4], they were divided into two groups: USIGP group (n=136) with GP and USI, and USI group (n=132) only with USI. Additionally, we divided the USIGP group into two subgroups: USIGP (A) (n=78) with GP stage I and USIGP(B) (n=58) with GP stage II. All participants were aware of group assignment. All subjects were given an explanation of the study and provided written informed consent.
Demographic data were measured, such as age, duration of postmenopausal age, parity, sport, diet, profession, and body mass index. Complete evaluation for GP consisted of a structured questionnaire and POP-Q during a pelvic examination performed in the supine position in a birthing chair in the rest position (RP) and while performing the Valsalva maneuver (VM) with maximal effort. The bladder was emptied by catheterization and the rectum also by morning defecation. Ultrasound evaluation of the lower urinary system was carried out with a perineal ultrasound probe of 3.5 MHz according to the "Recommendations of the German Association of Urogynecology on Functional Sonography of the Lower Female Urinary Tract" [1]. We oriented the picture so that it depicted the cranial parts above and the ventral parts on the right side. The measurement methods for the BN position were performed by using a rectangular coordinate system that was set up with the origin at the lower symphysis border as follows: 1) the x-axis was determined by the symphysis central line, which ran between its lower and upper borders, and 2) the y-axis was constructed perpendicular to the x-axis at the lower symphysis border. The following values were measured during three positions, i.e., in the RP, with maximal pelvic floor contraction (MPFC), and during VM: 1) Dx, as the distance between the BN and the y-axis during VM (Vx), in RP (Rx), and during MPFC (Cx); 2) Dy, as the distance between the BN and the x-axis during VM (Vy), in RP (Ry), and during MPFC (Cy); 3) the Sy-BN distance in the three positions, as the distance between the BN and the inferior symphysis border; 4) distance H (the height of BN), determined as the distance between the BN and the horizontal line, which is drawn at the lower symphysis border; 5) distance R→V, as the square root of the sum (Vx-Rx)2+(Ry-Vy)2; 6) angle of rotation (ρ), as the value (cotangent Ry/Rx)-(cotangent Vy/Vx); 7) pubourethral angle (α), as the angle between the distance Sy-BN and the x-axis; 8) retrovesical angle (β), as the angle in which one side lies along the line connecting the dorsocaudal and proximal urethra and the other side is formed by the tangent along the bladder base. The distance R→V and angle of rotation (ρ) show the BN movement and its rotation during VM. In Fig. 1, we present the ultrasound measurements in the USIGP group, and in Fig. 2 we present the measurements in the USI group in the three positions.
1. Statistical methods
The Student's paired t-test was used to compare the demographic data and ultrasound parameters among the three positions in the groups as well as between every particular position of both groups. The Mantel-Haenzel's chi-square test was used for comparing the demographic data and urodynamic parameters according to the formula:

RESULTS
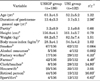
There were some significant differences in demographic data. For example, the postmenopausal age duration was longer in the USIGP group (p<0.01). Regarding professional occupation, the USIGP group was dominated by farmers and retired persons (p<0.05, p<0.001, respectively), whereas the USI group was predominantly factory workers and clerks or teachers (p<0.05, p<0.001, respectively) (Table 1).
Regarding POP-Q and its anatomical landmarks, there were differences between the groups, but also in the same group during the VM vs. the RP. Point Aa, which indicates the BN projection on the anterior vaginal wall midline, was situated higher in the RP but moved significantly lower during VM in the USI group than in the USIGP group (p<0.05). Point C, which represents the leading edge of the cervix, was situated significantly lower in the RP, and especially so during the VM, in the USIGP group than in the USI group (p<0.001, p<0.001, respectively). The total vaginal length (tvl) was significantly greater in the USI group than in the USIGP group in RP (p<0.05) (Table 2).
The differences in the ultrasound parameters are presented in Table 3. In the USI group we did not notice significant changes in any parameter during VM vs. RP. By contrast, in the USIGP group during VM vs. RP, we noticed a significant decrease of the α-angle and Sy-BN distance (p<0.025, p<0.01, respectively) and also a significant increase in the H distance (p<0.025). When we compared the groups, we found that 1) the α-angle was smaller in the USIGP group than in the USI group in RP, with MPFC, and during VM (p<0.025, p<0.01, p<0.001, respectively); 2) the β-angle was significantly greater in the USI group during VM (p<0.025); 3) the distance H was greater in the USIGP group than in the USI group during RP (p<0.025) and especially during VM (p<0.001); 4) the distance Sy-BN was significantly smaller in the USIGP group during VM (p<0.01); 5) the distance R→V and the angle of rotation (ρ) were greater in the USI group than in the USIGP group (p<0.01, p<0.001, respectively).
DISCUSSION
The significant decreases in the parameters a-angle and distance Sy-BN and also the significant increase in distance H that we found in the USIGP group during VM could be explained by an elevation of the BN owing to cystocele enlargement occurring in that position. On the contrary, in the USI group, we did not find significant changes in these ultrasound parameters, which could be explained by the slight mobility of the BN due to the intact pelvic floor, which is present in the absence of GP. The decreases in the parameters Dx and Dy during VM compared with RP in the USI group could be explained by an isolated deterioration of the pubo-urethral ligaments, which could in fact be the reason for the USI in these patients. These supportive structures are responsible for fixation of the urethra and BN to the posterior plane of the symphysis and for urinary continence during VM as well. On the other hand, regarding the ultrasound parameters that gave the best insight into the range of BN movements during VM, the distance R→V and angle of rotation (ρ), we found them to be significantly lower in the USIGP group (p<0.01, p<0.001, respectively). These findings could be evidence for the cystocele-immobilizing effect on the BN during the VM in the USIGP group, but also for the deterioration of the pubo-urethral ligaments in the USI group.
Sublimating the results from Table 2 (POP-Q with anatomical landmarks) and Table 3 (ultrasound parameters) in both groups, we constructed two models that could explain the possible movements of pelvic anatomical elements during the VM compared with RP. We present these possible models of movements in Figs. 3-5: 1) in Fig. 3 is shown the normal pelvic organ position in patients without USI and GP; 2) in Fig. 4 is shown the situation in patients in the USIGP group, who had concomitant USI and stage I/II GP; and 3) in Fig. 5 is shown the situation in patients in the USI group, in which isolated USI was present.
Chen et al. [5] assessed the differences in dynamic changes of the BN in 48 patients with or without urodynamic USI, comparing BN movement with computer-aided vector-based perineal ultrasound. Using corrected BN movement ≥10 mm as the cutoff point for diagnosis of USI, they found a sensitivity of 77.8%, specificity of 66.7%, positive predictive value (PPV) of 87.5%, negative predictive value (NPV) of 50%, and accuracy of 75% and concluded that this method was not a sensitive tool for predicting USI. Thompson et al. [6], assessing the movement of the BN and base during voluntary MPFC and VM in 60 asymptomatic and 60 incontinent women, found a strong trend for the continent women to have greater BN elevation (p<0.05). The incontinent women demonstrated increased BN descent during VM (p<0.001). In our study also, this trend of BN descent during the VM was present only in the USI group. On the contrary, the USIGP group showed an elevation of the BN during the VM. Bai et al. [7] investigated 164 women with USI and found BN hypermobility with a Q-tip angle ≥30° and significant BN descent with perineal ultrasound in 60% of patients. In our study, we found significantly greater mobility of the BN in the USI group than in the USIGP group, expressed with the following two ultrasound parameters: distance R→V and angle of rotation (ρ) (p<0.01, p<0.001, respectively). Huang et al. [8], who explored the correlation of anatomical/functional ultrasound parameters in 396 patients with urodynamic USI, found similar results, i.e., genitohiatal angle and genitohiatal distance were positively associated with BN funneling and dependent cystocele during stress but negatively with functional profile length. His results also could be explained with the present BN descent during the VM in patients with USI owing to deterioration of the pubo-urethral ligaments. According to Dietz [9], in patients with mild USI and anterior vaginal wall descent (cysto-urethrocele grade 2), the ultrasound image demonstrates the BN to be virtually part of the leading edge of the cystocele. On the contrary, in patients with cystocele and an intact retrovesical angle, the ultrasound image demonstrates the leading edge of the cystocele about 2 cm distal to the BN. These patients present with GP, but are often continent. Our results were similar to those of Huang et al. [8]. We also found a higher position of the BN during the VM in the USIGP group than in the USI group, expressed with the ultrasound parameters Dy and distance H. The patients in the USIGP group also were often continent during the VM, especially those in the USIPG(B) subgroup, who had a greater stage of GP (30/58, 51.72%). The pubourethral angle (α), which expresses the BN movement regarding the longitudinal central line of the symphysis (x-axis), was significantly higher in the USI group than in the USIGP group during the VM. Additionally, this parameter significantly decreased during the VM in the USIGP group, as a sign of the BN approaching the posterior symphysis plane during the VM. Similarly to Dietz [9], we found that in the USIGP group in which GP and cystocele were present, the ultrasound image demonstrated an intact retrovesical angle (β), i.e., it was significantly smaller in this group than in the USI group during the VM and these patients often were continent. Hajebrahimi et al. [10] found a significantly wider retrovesical angle (β) in patients with USI (n=40) compared with normal controls (n=40), as well as greater mobility of the urethra and BN. Minardi et al. [11] found that retrovesical-angle rotation and BN-descent during VM were strongly associated with genuine USI. In our study also, the distance R→V and angle of rotation (ρ), which expressed the mobility of BN, were greater in the USI group.
In our study, the clinical features (POP-Q with its landmarks) corresponded with ultrasound findings. Point Aa, which expresses the BN projection on the anterior vaginal wall midline, was situated higher during RP but moved significantly lower during VM in the USI group than in the USIGP group (p<0.05).
CONCLUSIONS
Point Aa, which is the BN projection on the anterior vaginal wall midline, was situated higher during RP but moved significantly lower during VM in the USI group than in the USIGP group (p<0.05). The decreases of the a-angle and distance Sy-BN, but also the increase in the distance H, in the USIGP group during the VM could be explained with a BN elevation due to cystocele enlargement during the VM. The two ultrasound parameters that gave the best insight into the range of BN movements during VM, i.e., the distance R→V and angle of rotation (ρ), were significantly higher in the USI group than in the USIGP group. These findings could be other possible evidence for the cystocele-immobilizing effect on the BN during the VM in the USIGP group and also for deteriorated pubo-urethral ligaments in the USI group.







 XML Download
XML Download