

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Boys with retractile testis are often transferred from primary health clinics because of suspected cryptorchidism [1]. In many studies, retractile testis is considered as a testis that is located at the upper scrotum or lower inguinal canal and that can be made to descend completely into the scrotum without resistance by manual reduction but returns to its original position by the cremasteric reflex [2-4]. Retractile testis has traditionally been considered as a variant of normal testis because it usually descends into the scrotum during adolescence and shows no difference in testicular volume or childbearing capacity compared with the normal testis [5]. In general, patients with retractile testis are periodically reviewed until the end of adolescence or until the testis has completely descended into the scrotum. However, surgical correction is necessary if testicular maturation appears to be poor or if the testis fails to descend into the scrotum and cryptorchidism develops secondarily.
Some previous studies conducted with boys with retractile testis reported that 18 to 32% of patients required surgical correction owing to the development of undescended testis or decreases in testicular volumes [6,7]. One study reported tissue degeneration among patients with retractile testis that was similar to that of undescended testis [8]. Another study suggested a possible relation between retractile testis and sterility owing to the fact that adults with retractile testis who receive follow-up care show abnormalities in semen analysis compared with normal adults [9]. Treatments of retractile testis remain controversial, but domestic research on the clinical follow-up of boys with retractile testis is insufficient. This study followed up and observed boys diagnosed with retractile testis to investigate the natural course of retractile testis and to analyze the need and the appropriate time of surgical treatments.
MATERIALS AND METHODS
Eighty-eight boys were transferred from primary health clinics to the department of urology in the hospital for suspected retractile testis or undescended testis between January 2001 and December 2008. Among them, 43 boys were included in this study who attended follow-up for longer than 1 year. Their medical records were retrospectively analyzed. Boys who underwent hormonal therapy were excluded.
Retractile testis was defined as a testis that was located in the upper scrotum or lower inguinal canal but that could be made to descend completely into the scrotum by manual reduction and then returned to the original position by the cremasteric reflex. Undescended testis was defined as a testis located in the upper scrotum or inguinal canal that could not be made to descend into the scrotum by manual reduction or that showed any resistance to reduction or returning immediately to its original position.
All patients were examined by a pediatric urologist. Their testicular location, mobility, and volume were compared with the results of their previous examination at the outpatient department every 6 months after the first diagnosis. According to testicular location, mobility, and volume, the patients were classified into the retractile testis, normal, and orchiopexy groups. Follow-up was terminated once the testis had descended into the scrotum or if any of the boys were diagnosed with undescended testis. Otherwise, the boys having retractile testis were subjected to further follow-ups. If testicular volume was smaller than the previously observed volume or smaller than that of the opposite testis, follow-up was also terminated owing to the judgment that testicular maturation had become poor. Testicular volume was measured with an orchidometer. Orchiopexy was performed for the boys whose testis had become undescended testis or whose testicular volume had decreased. We analyzed their long-term outcomes according to patients' age at the time of the diagnosis, testicular positions, and the status of the contralateral testis and changes in testicular volume.
One-way analysis of variance was used to compare the mean values of the normal, retractile, and orchiopexy groups and chi-square and linear-to-linear association tests were performed to analyze the categorical data. Results were considered to be significant if the p-value was less than 0.05.
RESULTS
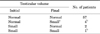
There were 22 boys (51.1%) with unilateral retractile testis and 21 boys (48.9%) with bilateral retractile testis among a total of 64 retractile testes. Of these 64 retractile testes, 29 cases (45.3%) succeeded in descending into the normal scrotum. By contrast, 9 cases (14.1%) underwent orchiopexy owing to decreased testicular volume (5 cases) or persistent undescended testis (4 cases). Twenty-six cases (40.6%) remained retractile testis until the end of adolescence. The mean follow-up period of the 43 boys was 4.4±1.7 years, and the mean follow-up period of the boys with persistent retractile testis until the last follow-up was 5.1±1.8 years. The mean diagnostic age was 3.0±2.7 years. The mean age of the patients whose testis succeeded in descending into the scrotum was 4.3±3.3 years, showing that it had taken an average of 4.0±1.4 years until their testis came to descend in the normal scrotum. By contrast, the mean age of the boys who underwent orchiopexy was 1.3±0.9 years, showing that it had taken an average of 3.6±1.5 years. The mean diagnostic age of the boys who underwent orchiopexy was significantly younger than that of the boys whose testis came to descend in the scrotum without surgical correction (p=0.009). There were no statistical differences according to position or bilaterality (p=0.284, 0.292) (Table 1).
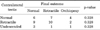
Among the total 64 cases, 61 cases showed normal volume and 3 cases had smaller volumes at the first diagnosis compared with the contralateral testis. According to the follow-up results, 4 cases among those 61 cases with normal volume showed a decrease in volume and underwent orchiopexy, whereas 57 cases maintained a normal volume. Among those 3 cases with smaller volumes, 2 cases recovered to a normal volume when the testis succeeded in descending into the normal scrotum, whereas 1 case showed a decrease in volume and underwent orchiopexy (Table 2).
The authors subdivided the subjects into 3 groups according to the status of the contralateral testis. Among the total 43 boys, 17 boys had a unilateral retractile testis and normal opposite testis, 21 boys had bilateral retractile testis, and 5 boys had a unilateral retractile testis and undescended opposite testis that previously underwent surgical correction. Of the 17 boys with unilateral retractile testis and normal opposite testis, 4 boys (23.5%) underwent orchiopexy, 8 boys (47.1%) came to have descended testis, and the other 5 boys (29.4%) continued to have retractile testis. Of the 5 boys with unilateral retractile testis and undescended opposite testis, 1 patient (20%) underwent orchiopexy, 3 patients (60%) came to have descended testis, and 1 patient (20%) continued to have a retractile testis. Of the 21 boys with bilateral retractile testis, 2 patients (9.5%) underwent orchiopexy for bilaterally persistent undescended testis, 9 patients (42.9%) came to have both testes in the scrotum, and 10 patients (47.6%) continued to have bilateral retractile testis. There was no statistically significant difference between the 3 groups (p=0.611) (Table 3).
DISCUSSION
Management methods for retractile testis remain controversial, whereas treatment methods for undescended testis have been well established through many studies [10-12]. It has been reported that retractile testis is accompanied by histological changes; abnormality on semen analysis was found during follow-up when patients with retractile testis became adults [8,9]. In addition, La Scala and Ein [7] reported that boys with retractile testis need periodic follow-up.
Testicular maturation requires a 2℃ to 4℃ lower temperature than the normal core body temperature of 36.5℃, and a normal scrotum can meet such a requirement by protrusion. However, a retractile testis goes up and down between the inside of the normal scrotum and the inguinal canal, and the temperature of the inguinal canal exerts an adverse effect on testicular maturation because it is close to the core body temperature. It is difficult, however, to accurately assess how long the testis stays inside the normal scrotum or in the upper scrotum. Therefore, it is essential to examine testicular volume and any changes affecting testicular maturation during the follow-up of patients with retractile testis. If there is any decrease in testicular volumes, immediate surgical correction will be required. It has been reported that a shrunken testis can recover to the normal level of testicular volume after surgical correction [13,14]. This result implies that the appropriate decrease in the temperature around the testis after surgical correction allows for testicular maturation. In this study, 4 of 9 patients underwent surgical correction after showing shrinkage of the ipsilateral testis compared with the contralateral testis or compared with the results of the previous physical examination before surgery. All 4 of these cases showed testicular growth after surgical correction, resulting in testicular volumes similar to those of the contralateral testis. Surgical correction is also required if the following abnormalities are detected during the physical examination. First, an undescended testis that fails to descend into the normal scrotum is developed; second, the development of a sliding testis secondary to increased spermatic cord tension in which the testis can descend into the normal scrotum but immediately returns to the original position; and finally, the development of pain during the descent of the testis, although the testis can descend into the normal scrotum [3]. In this study, 4 boys showed failure of complete descent and subsequently developed undescended testis during the follow-up period; therefore, they underwent orchiopexy.
There are contradictory results concerning histological changes in a retractile testis. Some previous studies reported that the retractile testis had the histological structure of the normal testis [4,15], whereas recent studies showed conflicting results. Recent studies have suggested that surgical correction is necessary to prevent histological changes if patients with retractile testis develop undescended testis [8,16,17]. However, according to research that investigated the testicular volumes and childbearing capacity of adults who had a medical history of retractile testis in both testes but did not undergo surgical correction, these variables were similar to those of a control group [18].
This study showed that a large number of boys with retractile testis diagnosed at a younger age tended to develop undescended testis, whereas none of the subjects diagnosed at the age of 6.5 years or older underwent surgical correction. Agarwal et al. [6] reported a similar result, claiming that the risk of development of undescended testis was higher in boys younger than 7 years old. However, this study included only 8 boys whose age was 6.5 or older at the time of the diagnosis. Therefore, further research with larger samples will be required in the future.
Previous studies showed that between 6.9% and 32% of boys with retractile testis require orchiopexy; in particular, 50.8 to 56% of boys with any resistance of the spermatic cord require orchiopexy [6,7,19]. The ratio of the boys who underwent orchiopexy in this study was 16.3%. A testis with any resistance against manual reduction was considered an undescended testis in this study. In previous studies, undescended testis was often misdiagnosed as retractile testis, which was subject to follow-up. This suggests that it is highly possible that the total sum of surgical candidates among patients with retractile testis may be much larger than the actual number. This result implies that care should be taken during the examination of patients with retractile testis to make a differential diagnosis with undescended testis. Much research has shown that a retractile testis may become an undescended testis during follow-up and annual or biannual follow-up for boys with retractile testis has been recommended [3,6,20]. In this study, the ratio of boys requiring orchiopexy for any reason was 16.3%. Therefore, we also agree with this recommendation that patients with retractile testis be examined closely concerning testicular location or volume until the testis has completely descended into the scrotum.
In addition, this study also analyzed outcomes according to the status of the contralateral testis. Agarwal et al. [6] reported that boys with 1 descended and 1 retractile testis had a higher probability for the retractile testis to be descended and boys with 1 undescended and 1 retractile testis had a higher probability for the retractile testis to be remained undescended. However, in this study, there was no significant difference in descent according to the status of the contralateral testis. All bilateral retractile testes had similar outcomes.
Hormonal therapy with human chorionic gonadotropin or gonadotrophin-releasing hormone is the most common treatment for undescended testis [21,22]. The action of hormones is similar to that of luteinizing hormones leading to a stimulation of the testis; the testis may then descend as it grows [23,24]. However, proof of the efficacy of hormonal therapy for undescended testis is limited as yet. There was a report that the practice of hormone therapy for less than 1 week was almost not effective for boys with unilateral undescended testis although it was found to be effective in about 56% of boys with bilateral undescended testis [25]. A number of studies have been conducted regarding hormone therapy among patients with retractile testis, and testicular descent was achieved by short-term hormone therapy. However, although short-term hormone therapy was effective, the therapy failed to prevent the return to retractile testis during follow-up [26]. Miller et al. [27] reported a response rate to hormonal therapy of 58% in a study conducted with 26 retractile testes among 16 patients and a response rate of 40% among patients with a retractile testis located in the inguinal canal. Boys who underwent hormonal therapy were excluded from the present study, because the aim of this study was to investigate the natural course of retractile testis. The rate of natural descent of the retractile testes located in the inguinal canal was 49.2% in this study.
This study demonstrated that boys who were diagnosed with retractile testis at a younger age were more likely to undergo orchiopexy. The status of the contralateral testis and testicular positions had no correlation to orchiopexy. Therefore, we suggest that boys with retractile testes, especially those diagnosed at a younger age, need closer observation and more frequent follow-up (annually or semiannually).
The limitations of this study include the error of selecting boys through retrospective investigations; the lack of a random design; judgements based only on physical examination without testicular biopsy; and the lack of complete follow-up until the end of adolescence in some boys. Other limitations are that the number of boys involved in the research was not large enough and that the results do not reflect the progress of patients who failed to attend the follow-up. Future research can address such limitations by involving a larger number of patients in a multi-center study that would allow the investigation of more details concerning the natural course of retractile testis.
CONCLUSIONS
About 16.3% of the boys diagnosed with retractile testis required surgical correction during long-term follow-up. The risk of orchiopexy was higher in the population diagnosed at a younger age. Judging from the results of this study, retractile testis might be considered as a variant of normal testis. Yet, close observation regarding testicular position, mobility, and volume through periodic follow-up is necessary until the testis has successfully descended into the scrotum or until the end of adolescence.

 XML Download
XML Download