

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In recent years, robot-assisted laparoscopic radical prostatectomy (RALRP) has become a widely accepted surgical alternative for the treatment of prostate cancer [1]. During RALRP, multiple modalities are used for hemostasis. The use of Hem-o-lok clips (HOLC; Weck Surgical Instruments, Teleflex Medical, Durham, NC, USA) is well documented for the lateral pedicles of the prostate during RALRP. Here we report the first case of bladder migration of HOLC without stone formation after RALRP.
CASE REPORT
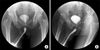
A 61 year old man presented to our institution with a diagnosis of stage T3a prostate cancer. His serum prostate-specific antigen level was 5.3 ng/ml, and a transrectal biopsy demonstrated a Gleason score of 3+4=7 in 20% to 80% of the cores from both lobes. After discussion of his prognosis and treatment options, he elected to undergo RALRP. A combination of suture ligation, bipolar cautery, harmonic scalpel, and HOLC were successfully used at various stages of the procedure to help achieve hemostasis and for ligation of the vas deferens. HOLC were used specifically for control of the lateral pedicle of the prostate during RALRP. We did not use HOLC at the bladder neck or the site of vesicourethral anastomosis. The vesicourethral anastomosis was achieved by using a single intracorporeal knot running 2-0 Monocryl suture. The procedure was uneventful, proceeding in the usual fashion without complications. There were no differences in the procedure compared with other patients undergoing RALRP. Also, the patient did not undergo wide dissection of the bladder neck during RALRP. Pathology showed a Gleason score of 3+4=7 with extracapsular extension, but negative lymph nodes, negative margins, no seminal vesicle invasion, and no angiolymphatic invasion. His postoperative recovery course was unremarkable. His Foley catheter was removed 1 week after surgery. Three months after surgery, he complained of dysuria and decreased force of the urine stream. He underwent retrograde cystourethrography in the office, which revealed a bladder neck contracture on the urethra (Fig. 1). He underwent urethral dilation with a guide wire for bladder neck contracture under cystourethroscopy. The cystourethroscopy demonstrated a normal-looking urinary sphincter but a very tight bladder neck. The bladder neck was successfully dilated, and visualization of the bladder revealed the presence of four HOLC. The four HOLC were floating in the bladder without stone formation and had migrated from the previous RALRP (Fig. 2). The clips were removed by use of a cystoscopic procedure (Fig. 3). After the procedure, an indwelling urethral catheter was left for 7 days. At the 3 month follow-up after this dilatation, the patient was satisfied with his voiding habits and reported having a good urinary stream.
DISCUSSION
With the recent surge in minimally invasive surgery (robotic and laparoscopic assisted surgery), interest in hemostatic alternatives to suturing has increased. Several automated suturing devices including EndoStitch (AutoSuture, USSC, Norwalk, CT, USA), LapraTy clips (Ethicon, Endosurgery Inc, Piscataway, NJ, USA), and HOLC have been used during laparoscopic procedures [2]. Among them, HOLC are a commonly used device and have been shown to be safe and reliable for vascular control in laparoscopic procedures [3]. During RALRP, HOLC have been used for ligation of the vasa deferentia, seminal vesicle arteries, and prostatic pedicles to prevent excessive electrocautery and possible injury to the neurovascular bundles [4]. However, several limitations, in addition to the concern for clip migration, have become apparent. Excessive clip usage in a narrow pelvis can limit visualization and mobility during RALRP. Another concern is the potential for an inflammatory reaction near the neurovascular bundles. The majority of reported complications with HOLC are clip migration and bladder neck contracture [5]. Blumenthal et al. [4] reported the first case of migration of HOLC into the vesicourethral anastomosis after RALRP. There have been some reports of intravesical migration of these clips causing urethral erosion, bladder neck contractures, and subsequent calculus formation [2-6]. In all those cases, however, HOLC lodged in the bladder neck area with stone formation. In our case, the HOLC were floating in the bladder without stone formation.
The mechanism underlying the migration of a surgical clip into the bladder is unclear [7]. There was also a recent report by Kadekawa et al. [8] of a case in which a metal clip had migrated into the urinary bladder after retropubic radical prostatectomy. It was hypothesized that inflammation had arisen around the urinary bladder or vesicourethral anastomosis and that this also involved the metal clip, which then eroded the bladder wall and eventually migrated into the bladder. Also, in our case, the mechanism of migration of HOLC in the bladder is unclear. According to the hypothesis described above, we can suspect that the HOLC migrated into the bladder during the serial course.
On the basis of these findings, we recommend minimizing the use of HOLC on tissue immediately adjacent to the anastomosis during RALRP, specifically, the vasa and seminal vesicles, and every effort should be made to retrieve any loose clips after the procedure. These clips are prone to migration and may cause, or significantly contribute to, bladder neck contracture formation after RALRP. Migration of HOLC into the vesicourethral anastomosis should be considered in patients with symptoms consistent with bladder neck contracture after RALRP. In addition, in these cases, noncontrast computed tomography scan might be helpful to detect clips.


 XML Download
XML Download