

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bladder cancer is the second most common genitourinary tumor in human populations, and it was estimated in 2012 that 73,510 new cases of cancer of the urinary bladder were diagnosed in the United States and 14,680 deaths were attributable to bladder cancer [1]. In Korea, bladder cancer is also the second most common urological malignancy and is about five times more common in men than in women [2,3]. Urothelial carcinoma of the bladder is classified as either non-muscle-invasive bladder cancer (NMIBC) or muscle-invasive bladder cancer (MIBC) on the basis of pathology and clinical behavior [4]. Although only 20% of bladder cancer patients are diagnosed with MIBC, the vast majority of cancer-specific deaths are due to MIBC, which leads to local invasion and distant metastasis. Although radical cystectomy is considered the gold standard for treatment of patients with localized MIBC, about 50% of such patients develop metastases within 2 years after cystectomy and subsequently die of the disease [5,6].
Bladder cancer has diverse biological and functional characteristics. Conventional histopathological evaluation, such as tumor stage or grade and lymph node status and numerous biomarkers have been investigated as prognostic indicators of MIBC [7,8]. However, none of the histological criteria or biomarkers reported to date have sufficient sensitivity and specificity for detecting the whole spectrum of bladder cancer diseases in a routine clinical practice [9]. The limited value of the established prognostic markers requires the analysis of new molecular parameters in predicting the prognosis and treatment of bladder cancer patients. Recently developed micro-array technology has permitted the development of numerous cancer classifiers, identification of tumor subclasses, discovery of progression markers, and prediction of disease outcome in many types of cancer [10-12]. Molecular staging may provide more accurate predictions of patient outcome than is currently possible with histopathological staging. Also, molecular staging could improve the treatment of patients by allowing treatment to be tailored to the severity of the disease. Although considerable effort has been devoted to identifying a prognostic model of MIBC that can provide useful information about survival and treatment options at diagnosis, the ability to predict the survival of MIBC patients remains a major clinical challenge. Thus, there is a critical need for methods capable of assessing the prognosis of patients with MIBC [13].
We have bladder cancer micro-array data and we have investigated genetic signatures associated with disease progression in patients with bladder cancer [7,13-15]. From previously published micro-array data, we found a new gene predicting cancer-specific survival in patients with MIBC. In this study, we validated this newly identified gene, FAM70B, as a prognostic marker in patients with MIBC by using techniques for quantifying RNA expression in a relatively large-scale, long-term, follow-up independent study population.
Go to : 
MATERIALS AND METHODS
1. Bladder cancer micro-array data
Micro-array gene-expression profiling techniques were described in previous reports [7]. In brief, we used 165 primary bladder cancer samples, 23 recurrent non-muscle-invasive tumor tissues, 58 normal-looking bladder mucosa surrounding cancer, and 10 normal bladder mucosa for micro-array analysis. Hierarchical clustering was used to stratify the prognosis-related gene classifiers. The full micro-array data set is available online at http://www.ncbi.nlm.nih.gov/geo/ under the data series accession number GSE13507.
2. Patients and tissue samples
Sixty-two patients with MIBC were selected by micro-array profiling (original cohort). We collected new tumor specimens from 124 MIBC patients with histologically verified urothelial cell carcinoma as a validation cohort. To reduce confounding factors affecting the analyses, and to delineate a more homogeneous study population, any patients diagnosed with a concomitant carcinoma in situ or for whom data collection was incomplete were excluded. All tumors were macro-dissected, typically within 15 minutes of surgical resection. Each bladder cancer specimen was confirmed by pathological analysis of a part of the tissue sample in fresh-frozen sections from cystectomy and transurethral resection (TUR) specimens, then frozen in liquid nitrogen and stored at -80℃ until use. The collection and analysis of all samples was approved by the Institutional Review Board of Chungbuk National University (IRB approval number 2006-01-001), and informed consent was obtained from each subject.
Tumors were staged according to the 2002 tumor-node-metastasis (TNM) classification and the 1973 World Health Organization grading system, respectively [4,16]. All diagnoses were confirmed by pathological analysis of frozen sections from cystectomy and TUR specimens. Patients with localized or locally advanced tumors and good Eastern Cooperative Oncology Group (ECOG) performance status (0 or 1) underwent radical cystectomy and complete pelvic lymph node dissection. Patients who were not eligible for radical cystectomy owing to metastatic disease, poor life expectancy, or poor ECOG performance status (≥2) underwent TUR for histopathological diagnosis. Patients with pT3, pT4, or node-positive disease according to the analysis of radical cystectomy specimens, or with metastatic disease but good performance status, received at least four cycles of cisplatin-based chemotherapy. Each patient was followed and managed according to standard protocols [17]. In this study, progression was defined as local regional recurrence or new distant metastasis in the cystectomized group and a ≥20% increment of mass or new distant metastasis in the noncystectomized group.
3. RNA extraction and construction of cDNA
One milliliter TRIzol (Invitrogen, Carlsbad, CA, USA) was added to bladder cancer tissue and homogenized in a 5-ml glass tube. The homogenate was transferred to a 1.5-ml tube and was mixed with 200 µl chloroform. After incubation for 5 minutes at 4℃, the homogenate was centrifuged for 13 minutes at 13,000×g at 4℃. The upper aqueous phase was transferred to a clean tube and 500 µl isopropanol was added, followed by incubation for 60 minutes at 4℃. The tube was then centrifuged for 8 minutes at 13,000×g and 4℃. Then, the upper aqueous phase was removed, mixed with 500 µl of 75% ethanol, and centrifuged for 5 minutes at 13,000×g and 4℃. After the upper aqueous layer was discarded, the pellet was dried at room temperature, dissolved with diethylpyrocarbonate-treated water, and stored at -80℃. The quality and integrity of RNA were confirmed by agarose gel electrophoresis and ethidium bromide staining, followed by visual examination under ultraviolet light. The cDNA was then prepared from 1 µg of random priming by using a First-Strand cDNA Synthesis Kit (Amersham Biosciences Europe GmbH, Freiburg, Germany) according to the manufacturer's protocol.
4. Real-time polymerase chain reaction (PCR)
To quantify the expression levels of FAM70B, real-time PCR amplification was performed with a Rotor Gene 6000 instrument (Corbett Research, Mortlake, Australia). Real-time PCR assays using SYBR Premix EX Taq (Takara Bio Inc., Otsu, Japan) were carried out in micro-reaction tubes (Corbett Research, Mortlake, Australia). The primers used for amplifying FAM70B (220 bp) were 5'-CCC TCG CCC GCC TAC TAT-3' and 5'-GCT GGG CGG GGT TGT AGA-3'. The PCR reaction was performed in a final volume of 10 µl, consisting of 5 µl of 2x SYBR premix EX Taq buffer, 0.5 µl of each 5'- and 3'- primer (10 pmol/µl), and 1 µl of the sample cDNA. The product was purified with a QIAquick Extraction kit (QIAGEN, Hilden, Germany), quantified with a spectrometer (Perkin Elmer MBA2000, Fremont, CA, USA), and sequenced with an automated laser fluorescence sequencer (ABI PRISM 3100 Genetic Analyzer, Foster City, CA, USA). The known concentration of the product was 10-fold serially diluted from 100 pg/µl to 0.1 pg/µl. The dilution series of PCR products were used for establishing the standard curve of real-time PCR. The real-time PCR conditions were 1 cycle at 96℃ for 20 seconds, followed by 40 cycles of 3 seconds at 96℃ for denaturation, 15 seconds at 60℃ for annealing, and 15 seconds at 72℃ for extension. The melting program was performed at 72 to 95℃ with a heating rate of 1℃ per 45 seconds. Spectral data were captured and analyzed by using Rotor-Gene Real-Time Analysis Software 6.0 Build 14 (Corbett Research, Mortlake, Australia). All samples were run in triplicate. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was applied as an endogenous RNA reference gene. Gene expression was normalized to the expression of GAPDH.
5. Statistical analysis
To normalize the highly skewed distribution of FAM70B mRNA expression, the data were examined as the natural log. Patients were classified as having a high expression of FAM70B or low expression of FAM70B, with the median (115.8×104 copies/µl) of the mRNA expression as the cutoff value. The Kaplan-Meier method was used to estimate cancer-specific survival, and differences were assessed by using log-rank statistics. The prognostic value of FAM70B expression was analyzed by using univariate and multivariate Cox proportional hazard regression models. Statistical analyses were performed by using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA), and p-values of less than 0.05 were considered statistically significant.
Go to :
RESULTS
1. Cancer-specific survival-related gene classifier
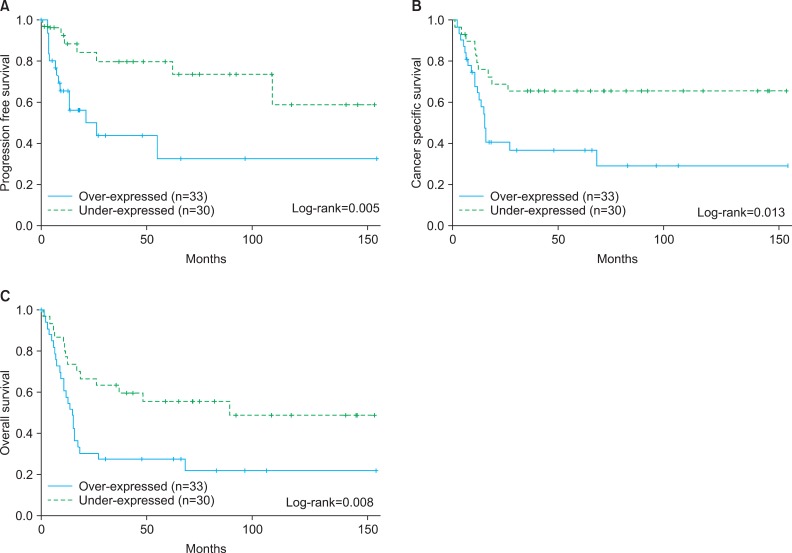
In the original cohort, FAM70B was associated with higher risk for cancer-specific death (hazard ratio [HR], 33.675; p<0.001), cancer progression (HR, 30.82; p=0.007), and overall survival (HR, 20.903; p=0.002) in patients with MIBC. Kaplan-Meier survival curves showing the effect of FAM70B expression on progression-free survival (log-rank test, p=0.005), cancer-specific survival (log-rank test, p=0.013), and overall survival (log-rank test, p=0.008) are shown in Fig. 1A, 1B, and 1C, respectively.
2. Baseline characteristics in the validation cohort and FAM70B mRNA expression stratified by clinicopathological parameters
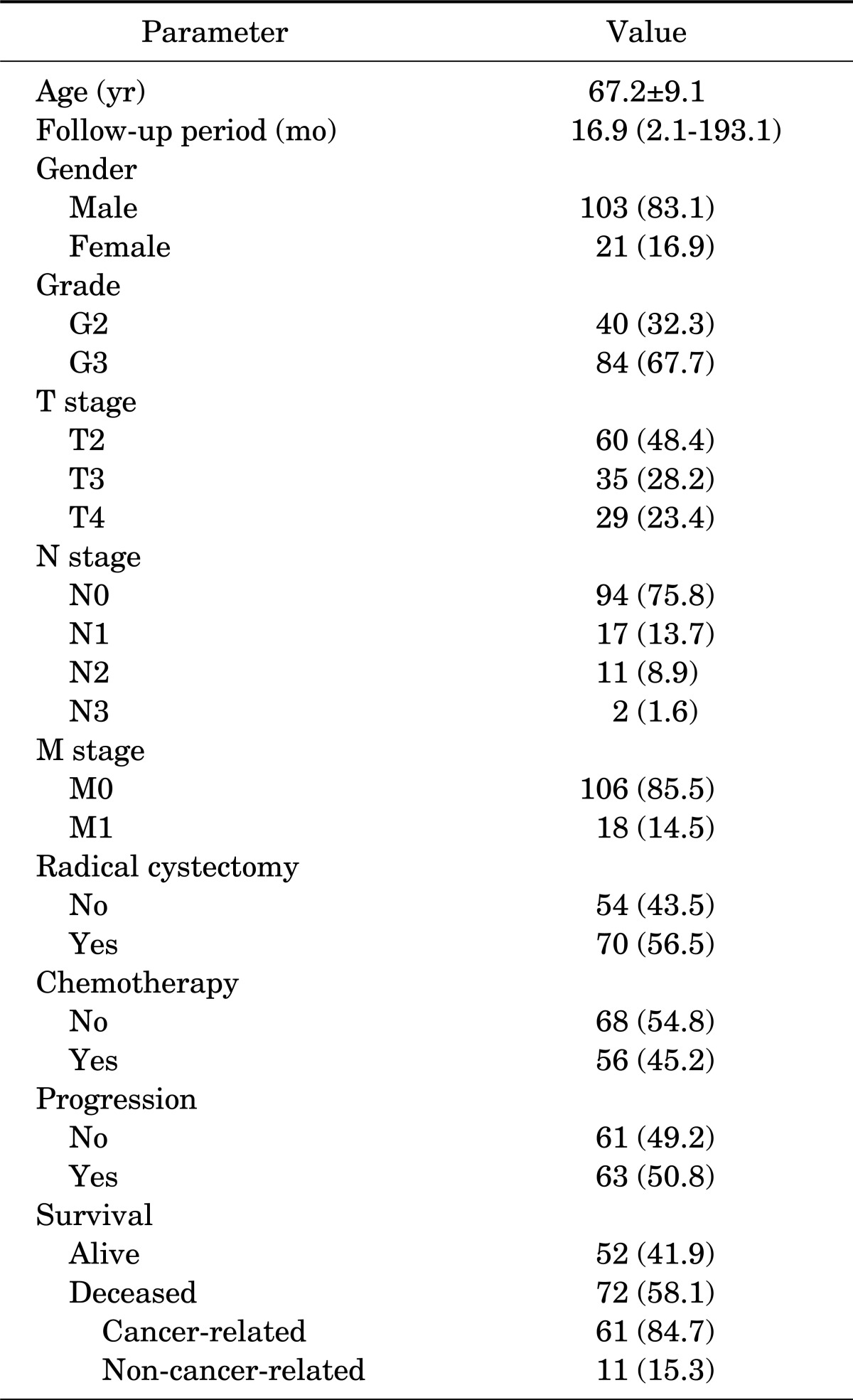
The baseline characteristics of the newly enrolled patients are listed in Table 1. Mean patient age was 65.2 years (range, 38 to 87 years) and mean±standard deviation follow-up was 37.8±45.9 months (median, 16.9; range, 2.1 to 193.1 months). A total 70 of 124 patients (56.5%) underwent radical cystectomy for MIBC. Other patients (43.5%) underwent TUR or biopsy for histopathological diagnosis. Systemic chemotherapy was performed in 56 patients (45.2%) after intervention. During the follow-up, 63 of 124 patients (50.8%) with MIBC experience progression and 61 (49.2%) died of their bladder tumor. Progression-free survival and cancer-specific survival were 32.9 months (median, 13.2 months) and 37.7 months (median, 16.9 months), respectively.
3. Predictive value of FAM70B expression for cancer prognosis
FAM70B expression and progression-free survival in MIBC
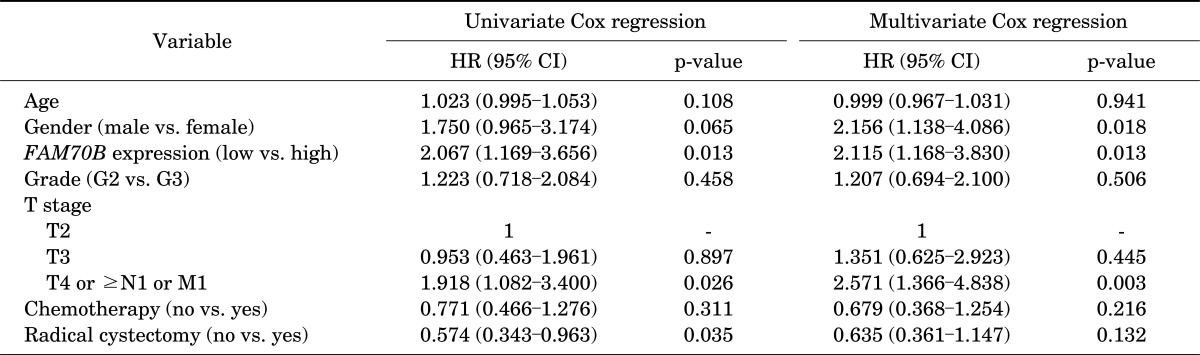
Kaplan-Meier estimates revealed significant differences in time for cancer progression according to FAM70B expression status. The patients with low FAM70B expression had significant progression-free survival benefits compared with those with high expression (log-rank test, p=0.011) (Fig. 2A). Univariate Cox regression analysis revealed that stage, radical cystectomy, and FAM70B expression each had a significant impact on the disease progression rate. In the multivariate analysis, gender (HR, 2.156; p=0.018), TNM stage T4 or ≥N1 or M1 (HR, 2.571; p=0.003), and FAM70B expression (HR, 2.115; p=0.013) were independent predictors of progression (Table 2).

FAM70B expression and cancer-specific death in MIBC
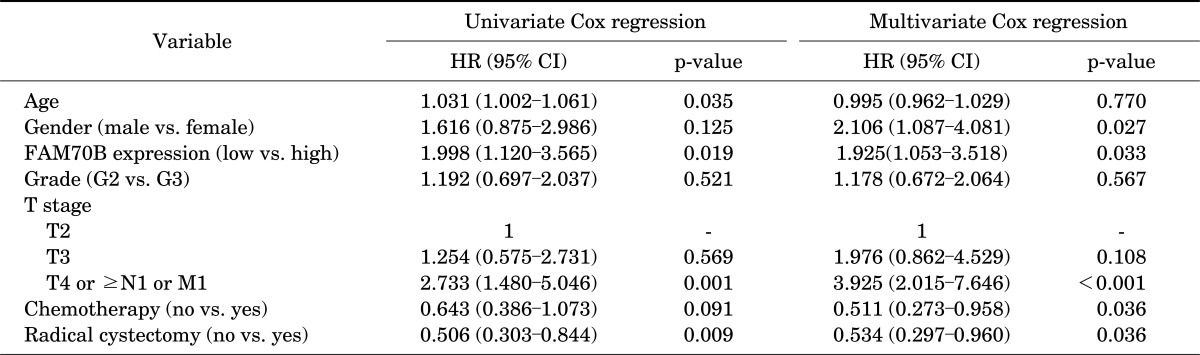
Kaplan-Meier estimates in the validation cohort revealed that patients with high FAM70B expression had significantly reduced cancer-specific survival compared with those with low FAM70B expression (log-rank test, p=0.017) (Fig. 2B). Age, TNM stage, radical cystectomy, and FAM70B expression each had a significant impact on the progression-free survival of MIBC patients by univariate analysis. In the multivariate analysis, gender (HR, 2.106; p=0.027), TNM stage T4 or ≥N1 or M1 (HR, 3.925; p<0.001), chemotherapy (HR, 0.511; p=0.036), radical cystectomy (HR, 0.534; p=0.036), and FAM70B expression (HR, 1.925; p=0.033) were independent predictors of overall survival (Table 3).
FAM70B expression and overall survival in MIBC
Kaplan-Meier estimates revealed no significant differences in overall survival of MIBC on the basis of FAM70B expression status (log-rank test, p=0.068) (Fig. 2C).
4. Predictive value of FAM70B expression for cancer prognosis according to cystectomy and chemotherapy status
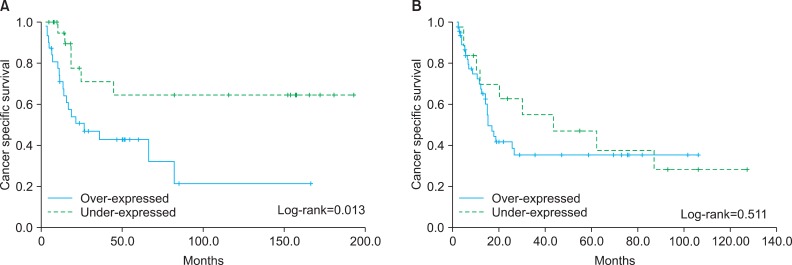
To create more homogeneous patient groups, patients were categorized according to chemotherapy and radical cystectomy status. In the patient group who underwent radical cystectomy, Kaplan-Meier estimates revealed a significant association between FAM70B expression and cancer-specific survival (log-rank test, p=0.013) (Fig. 3A). Similar results were identified in the chemotherapy group (log-rank test, p=0.013) (Fig. 4A). However, in the patient group who had not undergone radical cystectomy and had not received chemotherapy, FAM70B expression did not predict cancer-specific survival (Figs. 3B, 4B). Also, FAM70B expression successfully predicted progression-free survival and overall survival in MIBC patients who underwent radical cystectomy (log-rank test, p=0.036, p=0.005, respectively). In the chemotherapy group, FAM70B expression was associated with progression-free survival (log-rank test, p=0.042; data not shown).
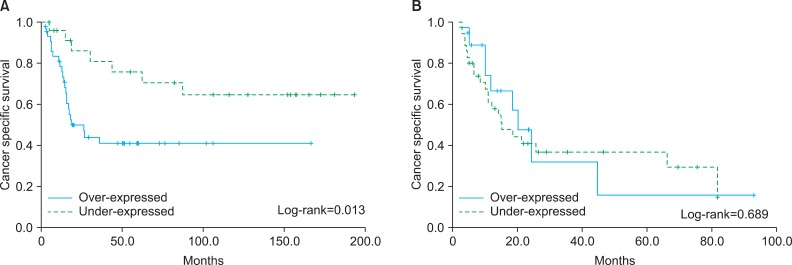 | FIG. 3Effect of FAM70B expression on cancer-specific survival of muscle-invasive bladder cancer patients, categorized according to radical cystectomy status. (A) Patients who underwent radical cystectomy (log-rank test, p=0.013). (B) Patients who did not undergo radical cystectomy (log-rank test, p=0.0689).
|
5. Predictive value of FAM70B expression for cancer prognosis according to TMN stage and tumor grade
Kaplan-Meier estimates revealed that FAM70B expression successfully predicted cancer-specific survival in the subjects with localized or locally advanced tumors (log-rank test, p=0.016) (Fig. 5A). In contrast, FAM70B expression was not associated with the cancer-specific survival in patients with tumor stage T4 or ≥N1 or M1 (log-rank test, p=0.372) (Fig. 5B).
 | FIG. 5Effect of FAM70B expression on cancer-specific survival of muscle-invasive bladder cancer patients, categorized according to tumor stage. (A) Patients with localized or locally advanced tumor stage (pT2-3N0M0) (log-rank test, p=0.016). (B) Patients with pT4 or node-positive or metastatic disease (log-rank test, p=0.372).
|
Go to :
DISCUSSION
The current study identified a gene expression signature associated with cancer progression and cancer-specific death in MIBC and demonstrated that this signature predicts the prognosis of MIBC. The gene network analysis suggests that a molecular mechanism involving genes might be responsible for cancer-specific death and cancer progression. The validity of this newly found gene as a prognostic indicator was confirmed in independent analyses of new MIBC cohorts. This study investigated the mRNA expression levels of FAM70B in human MIBC tissue, and our data showed a strong association between increased FAM70B mRNA expression and progression and cancer-specific death in patients with MIBC.
Bladder cancer is a genetic disorder driven by the progressive accumulation of multiple genetic and epigenetic changes [8,18]. At the molecular level, these genetic changes result in uncontrolled cell proliferation, decreased cell death, invasion, and metastasis. The specific alterations in gene expression that occur as a result of cross-talk between various cellular pathways determine the biological behavior of the tumor, including growth, recurrence, progression, and metastasis, and may influence patient survival. To detect and monitor cancer and determine the likely prognosis, it is necessary to identify molecular markers of the disease that can be used in the clinic. The advent of high-throughput microarray technology makes it possible to gain comprehensive insights into the molecular basis of numerous human diseases [19,20]. Micro-array gene expression analysis could be used to facilitate the identification of molecular prognostic markers that correlate with outcomes of numerous malignancies [21-26]. With this technology, hundreds or even thousands of genes in a tumor can be evaluated simultaneously, and individual molecular targets or gene classifier sets that correlate with particular bladder cancer outcomes can be identified. These studies open up the possibility of rapidly assessing gene expression patterns in individual tumors to determine tumor classification or to predict clinical outcomes and response to therapy [10,11,15,27].
The present study was designed to assess the independent prognostic utility of FAM70B in MIBC patients with a focus on cancer progression, cancer-specific survival, and overall survival. Kaplan-Meier estimates revealed the patients with low FAM70B expression had significant progression-free survival and cancer-specific survival benefits compared with those with high expression. Multivariate analysis showed the FAM70B was an independent predictor of cancer progression and cancer-specific death. Because radical cystectomy and chemotherapy are the most influential prognostic factors for MIBC, we performed a subgroup analysis to create more homogeneous patient groups. In the patients who underwent radical cystectomy or received chemotherapy, FAM70B expression was identified as a reliable biomarker for predicting cancer-specific survival and progression-free survival. However, in the patient group who had not undergone radical cystectomy and had not received chemotherapy, FAM70B expression did not show a significant difference in prediction of survival. In the subgroup analysis according to tumor stage, FAM70B expression did not show a significant difference in prediction of cancer-specific survival in the subjects who had advanced or metastatic disease. Although we do not know the exact reason, one possibility is that the patient group who had not undergone cystectomy and had not received chemotherapy had a relatively poor life expectancy or relatively poor ECOG performance status. Thus, this gene did not influence survival-related prognosis in these patients.
FAM70B (official full name: family with sequence similarity 70, member B) was found as part of the results of the Human Genomic Project [28,29]. The locus of the gene is on chromosome 13q34, and its function is protein coding. The exact mechanism of action of the gene has yet to be characterized in the oncological research field. Although the exact function of this gene has not been determined, our study showed the usefulness of this gene as a potential prognostic marker for bladder cancer. Additional studies are needed to define the precise roles of FAM70B on tumorigenesis and metastasis in bladder cancer.
A possible limitation of the present study is that we did not evaluate the protein level of FAM70B, such as by Western blot or immunohistochemical staining. FAM70B is a newly found gene and no antibody is yet available. To overcome these concerns, our group is planning to collect more MIBC tissues and to cooperate with other research groups and companies to identify the function of this novel biomarker.
Go to :
CONCLUSIONS
This study showed that FAM70B is a promising biomarker for assessing the prognosis of patients with MIBC. Our data indicate that the expression level of FAM70B can be recommended as a useful marker for predicting disease progression as well as the cancer-specific survival of patients with MIBC. A functional study will be necessary to identify the function of the gene.
Go to :
 XML Download
XML Download